
Peer Reviewed
Diffuse Red Eruptions in a Young Boy
Correct answer: B. Pityriasis lichenoides et varioliformis acuta (PLEVA)
Discussion. PLEVA, also known as Mucha-Habermann disease, is a benign and uncommon cutaneous inflammatory disorder that is part of the disease spectrum of pityriasis lichenoides chronica.1 PLEVA can occur in people of all ages, but it tends to predominate in boys from late childhood to early adulthood.2 While the etiology is unknown, it has been hypothesized that PLEVA may be an inflammatory reaction triggered by foreign agents such as infections (eg, HIV, parvovirus B19) or medications (eg, estrogen-progesterone, tumor necrosis factor-α inhibitors, statins).1 It has also been postulated that PLEVA could be an inflammatory response to a T-cell dyscrasia or an immune complex mediated hypersensitivity.3 Febrile ulceronecrotic Mucha-Habermann disease (FUMHD) is a rare, severe, and potentially life-threatening variant of PLEVA, with a predominate T-cell infiltrate.1,4 Although the exact etiology is unknown, FUMHD has been regarded as a low-grade lymphoproliferative disorder.
PLEVA presents as an acute eruption of bright red inflammatory papules that rapidly evolve into small blisters and pustules, which eventually ulcerate and develop necrotic crusts.1,3,4 The lesions can appear individually or grouped and most commonly occur on the trunk, thighs, upper arms, and skin flexures. Mucosal sites are typically spared.4 PLEVA may be asymptomatic or associated with mild pruritus, burning, and rarely, fevers or arthralgias. Due to its relapsing and remitting nature, all stages of lesions may be represented on physical examination.
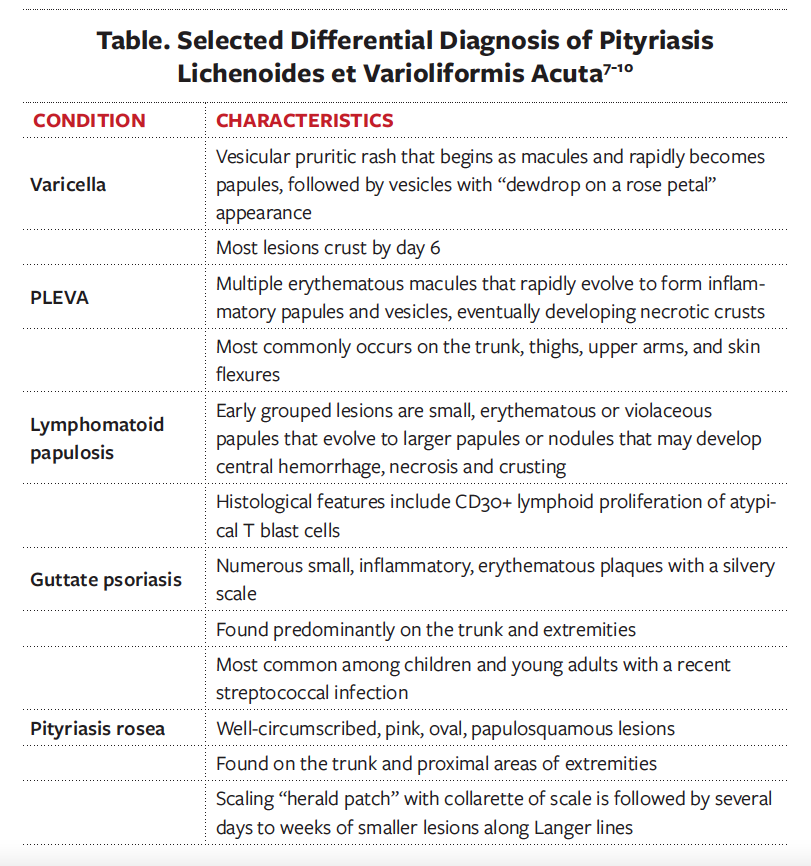
While a strong clinical suspicion is imperative, a skin biopsy allows for clinicopathological correlation to confirm the diagnosis of PLEVA and eliminate the differential diagnosis (Table). Although there are no pathognomonic histologic findings associated with PLEVA, common features such as vacuolar interface dermatitis and erythrocyte extravasation aid in the diagnosis.3,4

Because PLEVA is a self-limiting disorder, it will resolve without treatment but can last weeks to years. A course of antibiotics, such as erythromycin or tetracycline, and phototherapy are considered first-line treatments that can hasten the resolution of lesions. Topical corticosteroids may also be used to relieve symptoms, as well as methotrexate for patients who have failed previous treatment regimens.1,5,6
Varicella, though also an acute development of papulovesicles on multiple areas of skin, often presents as lesions that tend to be described as “dewdrop on a rose petal.” The course of disease is shorter than PLEVA, usually lasting only 1 to 2 weeks.7
Lymphomatoid papulosis most closely resembles PLEVA. While the cutaneous lesions are similar to lesions seen with PLEVA, the histologic features distinguish the two. Lymphomatoid papulosis is characterized by a dermal infiltrate composed of large atypical lymphocytic blast cells that are CD30+, which are rare in PLEVA. PLEVA also occurs more often in younger patients, is relatively short-lived, and rarely, if ever, progresses to lymphoma.8
Like PLEVA, guttate psoriasis most often presents in children and young adults and can be asymptomatic, pruritic, or painful. Unlike PLEVA, however, guttate psoriasis lesions emerge abruptly, usually 1 to 2 weeks after a streptococcal infection. The lesions are small, round, or oval erythematous plaques with a silvery scale. Furthermore, guttate lesions are often symmetrically distributed over the trunk and proximal extremities, differing from the pattern of presentation of PLEVA.9
Pityriasis rosea can mimic PLEVA in its early presentation. While PLEVA is more papulonecrotic with more persistent and recurrent lesions, pityriasis rosea is composed of scaly patches or plaques that tend to follow Langer lines.10
1. Wood GS, Reizner GI. Other papulosquamous disorders. In: Bolognia J, Schaffer JV, Cerroni L, eds. Dermatology. 4th ed. Elsevier; 2017:161-174.
2. Zang JB, Coates SJ, Huang J, Vonderheid EC, Cohen BA. Pityriasis lichenoides: Long-term follow-up study. Pediatr Dermatol. 2018;35(2):213-219. https://doi.org/10.1111/pde.13396
3. Pereira N, Brinca A, Manuel Brites M, José Julião M, Tellechea O, Gonçalo M. Pityriasis lichenoides et varioliformis acuta: case report and review of the literature. Case Rep Dermatol. 2012;4(1):61-65. https://doi.org/10.1159/000337745
4. Ediale C, Felix K, Anderson K, Ahn C, McMichael AJ. An atypical presentation of PLEVA: case report and review of the literature. J Drugs Dermatol. 2019;18(7):690-691. https://jddonline.com/articles/dermatology/S1545961619P0690X&download=1
5. Bellinato F, Maurelli M, Gisondi P, Girolomoni G. A systematic review of treatments for pityriasis lichenoides. J Eur Acad Dermatol Venereol. 2019;33(11):2039-2049. https://doi.org/10.1111/jdv.15813
6. Jung F, Sibbald C, Bohdanowicz M, Ingram JR, Piguet V. Systematic review of the efficacies and adverse effects of treatments for pityriasis lichenoides. Br J Dermatol. 2020;183(6):1026-1032. https://doi.org/10.1111/bjd.18977
7. Gnann JW Jr, Whitley RJ. Clinical practice. Herpes zoster. N Engl J Med. 2002;347(5):340-346. https://doi.org/10.1056/nejmcp013211
8. Moy A, Sun J, Ma S, Seminario-Vidal L. Lymphomatoid papulosis and other lymphoma-like diseases. Dermatol Clin. 2019;37(4):471-482. https://doi.org/10.1016/j.det.2019.05.005
9. Brandon A, Mufti A, Gary Sibbald R. Diagnosis and management of cutaneous psoriasis: a review. Adv Skin Wound Care. 2019;32(2):58-69. https://doi.org/10.1097/01.asw.0000550592.08674.43
10. Schadt C. Pityriasis rosea. JAMA Dermatol. 2018;154(12):1496. https://doi.org/10.1001/jamadermatol.2018.3290