
Peer Reviewed
Van der Woude Syndrome
AUTHORS:
Brina Bui, BA • Makenna Arca, BS • Lynnette J. Mazur, MD, MPH
AFFILIATION:
McGovern Medical School at UT Health, Houston, Texas
CITATION:
Bui B, Arca M, Mazur LJ. Van der Woude syndrome. Consultant. 2020;60(5):e11. doi:10.25270/con.2020.03.00020
Received November 19, 2019. Accepted February 28, 2020.
DISCLOSURE:
The authors report no relevant financial relationships.
CORRESPONDENCE:
Lynnette J. Mazur, MD, MPH, McGovern Medical School at UT Health, 6431 Fannin St, Houston, TX 77030 (lynnette.j.mazur@uth.tmc.edu)
On a medical mission to treat the indigenous Cabécar people of Costa Rica, a 4-year-old girl and her 15-year-old brother came to the pediatric clinic for a checkup. On physical examination, the girl had a well-healed cleft lip scar and lower lip pits, and her brother had lower lip pits with no other abnormalities. The children’s mother exhibited less-obvious lower lip pits (Figures 1-3).

Figure 1. A 4-year-old girl with well-healed cleft lip scar and lower lip pits.

Figure 2. A 15-year-old boy, the girl’s brother, with lower lip pits.

Figure 3. The children’s mother with less-obvious lower lip pits.
DISCUSSION
Van der Woude syndrome (VWS), first described in 1845, manifests clinically as lower lip pits and cleft lip and/or palate.1 It occurs in an estimated 3.6 per 100,000 live births, and it exhibits an autosomal dominant inheritance pattern with an estimated penetrance of 89% to 99% and variable expressivity.2,3
Approximately 70% of VWS cases are associated with deletions or mutations of the interferon regulatory factor 6 gene (IRF6) at 1q32-q41.4-7 Mutations in the grainyhead-like transcription factor 3 gene (GRHL3) have been identified in several families with VWS, providing evidence for locus heterogeneity.8
VWS is the most common cause of syndromic clefts and syndromic lip pits, accounting for 2% and 80%, respectively.7,9,10 Lower lip pits are the most common manifestation of VWS, and the lip pits range from subtle depressions to bilateral fistulae with or without drainage of minor salivary glands.1 VWS can also present with hypodontia, hypoplasia, ankyloglossia, high arched palate, limb anomalies, congenital heart defects, finger syndactyly, syngnathia, and ankyloblepharon.11,12
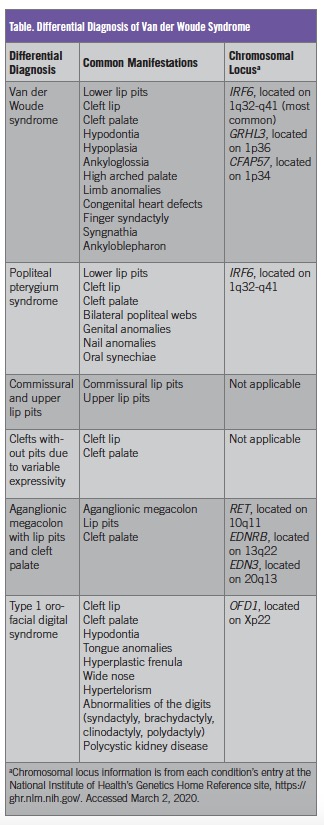
The differential diagnosis (Table) includes popliteal pterygium syndrome (PPS), commissural and upper lip pits, clefts without pits due to variable expressivity, aganglionic megacolon with lip pits and cleft palate, and type 1 orofacial digital syndrome.13 VWS and PPS are similar in that both can present with lower lip pits with cleft lip and/or palate. However, patients with PPS may also have bilateral popliteal webs, genital and nail anomalies, and oral synechiae. It is hypothesized that PPS and VWS are allelic variants of the same condition.14 Therefore, individuals with VWS can have children with PPS.
For children who present with signs and symptoms of VWS, a thorough orofacial examination must be performed to identify the type and extent of pitting and/or clefting. These patients may also have cardiovascular defects, so a thorough physical examination is also important. It is best to approach these patients with a multidisciplinary team including dentists, otolaryngologists, pediatric plastic surgeons, geneticists, genetic counselors, social workers, and occupational, speech, and physical therapists.
Pediatric plastic surgeons correct the cleft lip and/or cleft palate using the same approach as is used for nonsyndromic cleft lip and/or cleft palate. Lip pits can be removed during a minor surgical procedure in which saliva drainage is rerouted and lip aesthetics are improved. A pediatric geneticist is helpful in explaining the 50% risk of occurrence in the children of a patient with VWS.
REFERENCES:
- Kumaran S, Dogra S, Kanwar AJ. Van der Woude syndrome. Clin Exp Dermatol. 2004;29(4):434. doi:10.1111/j.1365-2230.2004.01556.x
- Burdick AB. Genetic epidemiology and control of genetic expression in van der Woude syndrome. J Craniofac Genet Dev Biol Suppl. 1986;2:99-105.
- Burdick AB, Bixler D, Puckett CL. Genetic analysis in families with van der Woude syndrome. J Craniofac Genet Dev Biol. 1985;5(2):181-208.
- de Lima RLLF, Hoper SA, Ghassibe M, et al. Prevalence and nonrandom distribution of exonic mutations in interferon regulatory factor 6 in 307 families with Van der Woude syndrome and 37 families with popliteal pterygium syndrome. Genet Med. 2009;11(4):241-247. doi:10.1097/GIM.0b013e318197a49a
- Leslie EJ, Mancuso JL, Schutte BC, et al. Search for genetic modifiers of IRF6 and genotype-phenotype correlations in Van der Woude and popliteal pterygium syndromes. Am J Med Genet A. 2013;161A(10):2535-2544. doi:10.1002/ajmg.a.36133
- Schutte BC, Basart AM, Watanabe Y, et al. Microdeletions at chromosome bands 1q32-q41 as a cause of Van der Woude syndrome. Am J Med Genet. 1999;84(2):145-150. doi:10.1002/(sici)1096-8628(19990521)84:2<145::aid-ajmg11>3.0.co;2-l
- Sander A, Schmelzle R, Murray J. Evidence for a microdeletion in 1q32-41 involving the gene responsible for Van der Woude syndrome. Hum Mol Genet. 1994;3(4):575–578. doi:10.1093/hmg/3.4.575
- Peyrard-Janvid M, Leslie EJ, Kousa YA, et al. Dominant mutations in GRHL3 cause Van der Woude syndrome and disrupt oral periderm development. Am J Hum Genet. 2014;94(1):23-32. doi:10.1016/j.ajhg.2013.11.009
- Koillinen H, Wong FK, Rautio J, et al. Mapping of the second locus for the Van der Woude syndrome to chromosome 1p34. Eur J Hum Genet. 2001;9(10):747-752. doi:10.1038/sj.ejhg.5200713
- Van der Woude syndrome. In: Wynbrandt J, Ludman MD. The Encyclopedia of Genetic Disorders and Birth Defects. 3rd ed. Facts on File; 2008:383.
- Deshmukh PK, Deshmukh K, Mangalgi A, Patil S, Hugar D, Kodangal SF. Van der Woude syndrome with short review of the literature. Case Rep Dent. 2014;2014:871460. doi:10.1155/2014/871460
- Schinzel A, Kläusler M. The Van der Woude syndrome (dominantly inherited lip pits and clefts). J Med Genet. 1986;23(4):291-294. doi:10.1136/jmg.23.4.291
- Rizos M, Spyropoulos MN. Van der Woude syndrome: a review. Cardinal signs, epidemiology, associated features, differential diagnosis, expressivity, genetic counselling and treatment. Eur J Orthod. 2004;26(1):17-24. doi:10.1093/ejo/26.1.17
- Lees MM, Winter RM, Malcolm S, Saal HM, Chitty L. Popliteal pterygium syndrome: a clinical study of three families and report of linkage to the Van der Woude syndrome locus on 1q32. J Med Genet. 1999;36(12):888-892.