
Peer Reviewed
An Atlas of Lingual Lesions, Part 2
Morphea (Localized Scleroderma)
Morphea, also known as localized scleroderma, is a distinctive chronic inflammatory disease that primarily affects the skin and underlying tissues, and ultimately leads to hardening and thickening of the skin due to excessive collagen deposition.1,2 The incidence of morphea is estimated to be approximately 0.4 to 2.7 cases per 100,000 population per year.3 The condition is more prevalent in white females.1,4 It has a bimodal peak age of onset, between 2 and 14 years and again between 40 and 50 years.3,4
Circumscribed or plaque morphea accounts for approximately 60% of cases in adults and 25% of cases in children.5 The condition typically presents as fewer than 3 oval or round, discrete, indurated plaques, confined to one anatomic area.5 The lesions occur most frequently on the trunk or proximal extremities (Figure 1).5 The face is one of the most common sites for the linear type of morphea.6 Uncommonly, morphea may occur on the tongue (Figure 2).6,7 The patient shown in Figure 2 had morphea affecting the left side of the chin, lower lip, and dorsal aspect of the tongue.
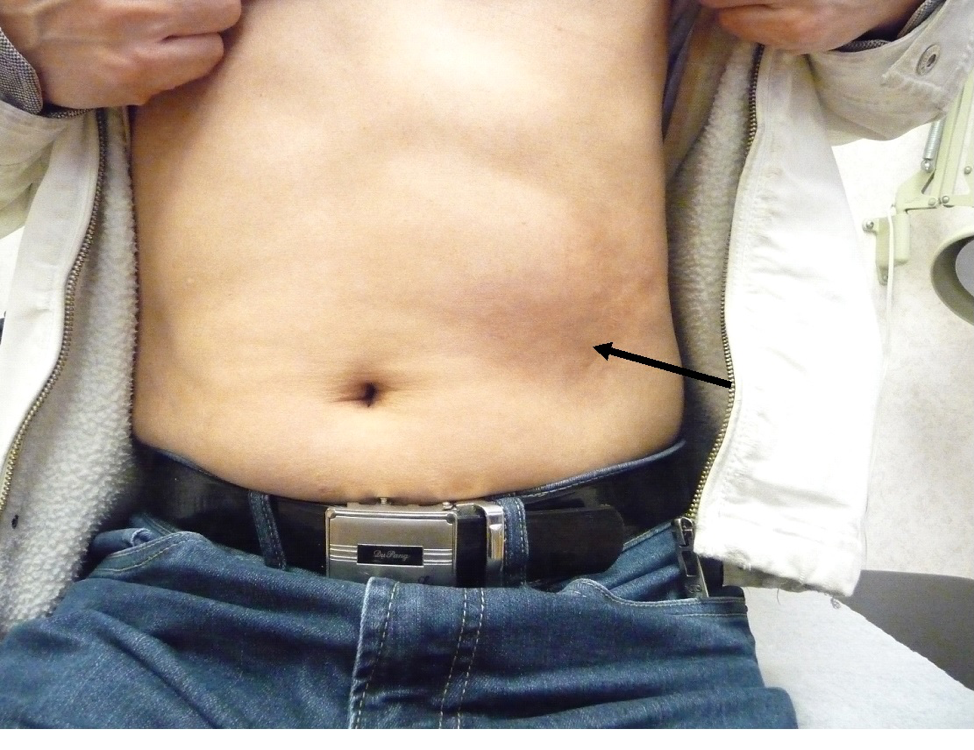
Figure 1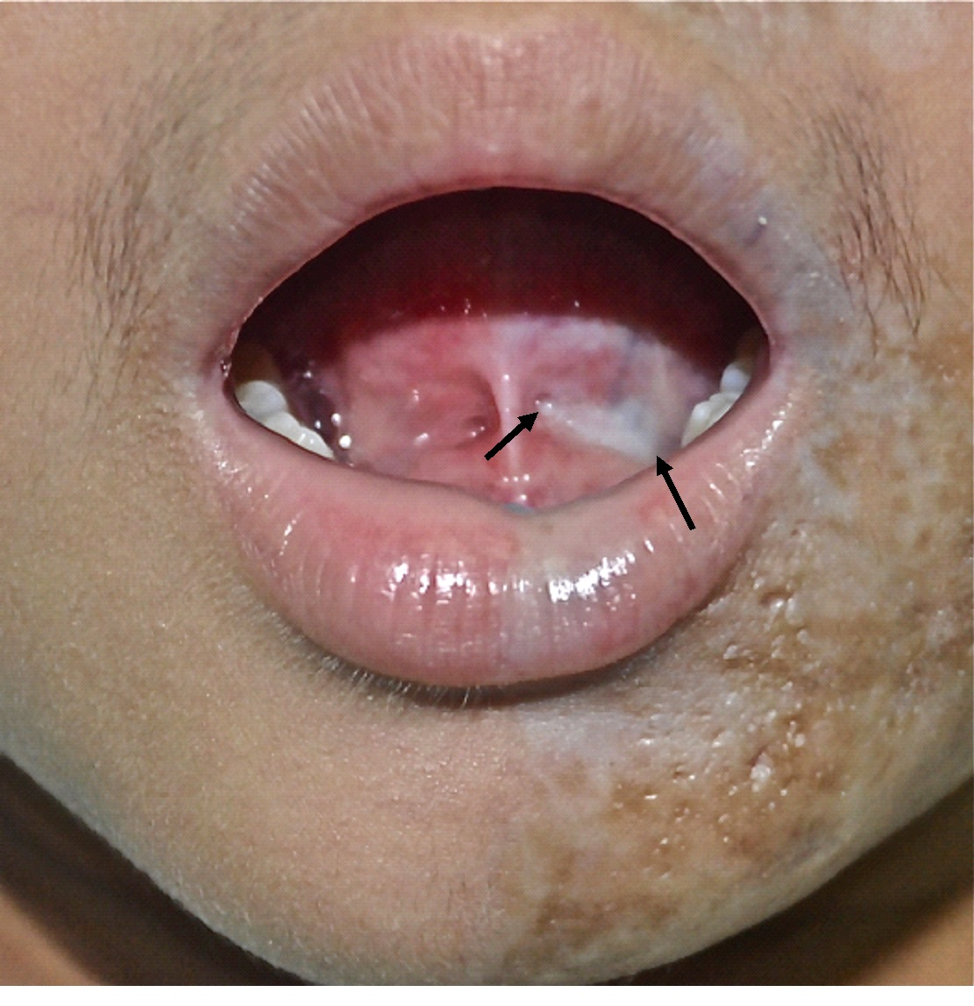
Figure 2The lesion typically begins as an erythematous or violaceous macule with a smooth surface and a yellowish white center. Over time, the lesion develops central sclerosis, which is ivory-white with surrounding erythema or violaceous hue and induration.2 Eventually, the sclerotic area becomes softened and atrophic with varying degrees of postinflammatory hypopigmentation/hyperpigmentation.8 The area is often hairless and anhidrotic.
The disease may cause functional and cosmetic impairment and may impair quality of life.2 Depression and anxiety may develop.3 If the lesion crosses a joint, it may lead to restriction of joint movement and joint contractures.5
The diagnosis is mainly clinical. The use of dermoscopy facilitates visualization of pigment network-like structures and fibrotic beams; the latter indicate sclerotic dermis.9 Those dermoscopic features are characteristic of morphea.9 A skin biopsy should be considered if the diagnosis is in doubt.
In general, lesions tend to run a waxing and waning course. Most lesions regress spontaneously over 3 to 5 years, usually with residual pigmentary and atrophic changes.3 Affected patients may develop new morphea lesions over their lifetime.2
Treatment should be individualized. For some patients with uncomplicated limited circumscribed morphea, treatment might not be necessary apart from reassurance.2 Other patients with circumscribed morphea with limited and superficial involvement may benefit from treatments with topical tacrolimus, topical corticosteroids, intralesional corticosteroids, topical imiquimod, and/or topical calcipotriene.2,8 Physiotherapy should be considered if the lesion involves a joint or if there is limitation of movement and/or joint contracture.1,3 Systemic therapies should be considered for patients with subcutaneous involvement, rapidly progressive disease, or involvement of large body surface area or functionally/cosmetically sensitive areas.2 Therapeutic options include systemic methotrexate, a systemic corticosteroid, and phototherapy, alone or in combination.2,8
REFERENCES:
- Bielsa Marsol I. Update on the classification and treatment of localized scleroderma. Actas Dermosifiliogr. 2013;104(8):654-666.
- Leung AKC, Barankin B. An adolescent whose “bruises” don’t fade: what is this patchy discoloration? Morphea (localized scleroderma). Consultant Pediatricians. 2015;14(9):402-406.
- Browning JC. Pediatric morphea. Dermatol Clin. 2013;31(2):229-237.
- Pope E, Laxer RM. Diagnosis and management of morphea and lichen sclerosus and atrophicus in children. Pediatr Clin North Am. 2014;61(2):309-319.
- Torok KS. Pediatric scleroderma: systemic or localized forms. Pediatr Clin North Am. 2012;59(2):381-405.
- Dixit S, Kalkur C, Sattur AP, Bornstein MM, Melton F. Scleroderma and dentistry: two case reports. J Med Case Rep. 2016;10(1):297.
- Tan E, Kürkçüoğlu N, Atalağ M, Gököz A, Zileli T. Progressive hemifacial atrophy with localized scleroderma. Eur Neurol. 1989;29(1):15-17.
- Jacobe H, Ahn C, Arnett FC, Reveille JD. Major histocompatibility complex class I and class II alleles may confer susceptibility to or protection against morphea: findings from the Morphea in Adults and Children cohort. Arthritis Rheumatol. 2014;66(11):3170-3177.
- Shim W-H, Jwa S-W, Song M, et al. Diagnostic usefulness of dermoscopy in differentiating lichen sclerosis et atrophicus from morphea. J Am Acad Dermatol. 2012;66(4):690-691.