
Pearls of Wisdom: Which Antihypertensive Is Best For Your Patient?
Geraldine, a 32-year-old woman, comes to your office with her 66-year-old grandmother. She tells you that Grandma “isn’t much for doctors.”
Despite Grandma’s protestations, Geraldine insists on getting her treatment for her blood pressure, which has consistently been 160/100 mm Hg or greater. She tells you that Grandma has restricted salt, is exercising, and her body mass index is 26.5. Geraldine puts it to you fairly simply: What medicine for blood pressure has the best effect on mortality?
Is there an antihypertensive agent that provides an advantage for reductions in mortality compared with other agents?
- Yes, ACE inhibitors reduce mortality more than other drugs
- Yes, thiazide diuretics reduce mortality more than other drugs
- Yes calcium channel blockers reduce mortality more than other drugs
- No, all 3 classes of agents reduce mortality equivalently
What is the correct answer?
(Answer and discussion on next page)
Louis Kuritzky, MD, has been involved in medical education since the 1970s. Drawing upon years of clinical experience, he has crafted each year for almost 3 decades a collection of items that are often underappreciated by clinicians, yet important for patients. These “Pearls of Wisdom” often highlight studies that may not have gotten traction within the clinical community and/or may have been overlooked since their time of publishing, but warrant a second look.
Now, for the first time, Dr Kuritzky is sharing with the Consultant360 audience. Sign up today to receive new advice each week.
Answer: No, all 3 classes of agents reduce mortality equivalently.
Hypertension is reported to be the most common medical disorder treated in the ambulatory setting.
The History of Hypertension Treatment
The treatment of hypertension was confirmed to be highly effective as early as the 1960s, at which time some experts were concerned that bringing down high blood pressure (BP) might be detrimental. The idea was that older persons with very high BP needed that degree of elevated pressure to perfuse their more rigid arterial system, and that reducing BP would induce ischemia.
__________________________________________________________________________________________________________________________________________________________________
RELATED CONTENT
Effects of Antihypertensive Drug Treatment on Cognitive Function
Hypertension: How to Treat the Elderly
__________________________________________________________________________________________________________________________________________________________________
By the 1990s, tens of thousands of participants in hypertension trials had established a consistent track record: the treatment of hypertension reduces incident myocardial infarction by about 25%, stroke by 35%, and heart failure by about 50%.
Investigators then turned their attention to the thorny question: If all of the antihypertensive agents work to reduce target organ damage and cardiovascular endpoints, which one is the best to start with?
The Research
The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) trial—the largest hypertension trial ever performed—was designed to answer that question.1
In the original trial there were 4 hypertension groups: ACE inhibitor (lisinopril), Diuretic (Chlorthalidone), Calcium Channel Blocker (amlodipine), and Alpha Blocker (doxazosin). The total population of the trial at inception was slightly over 44,000. Because every agent that reduces BP has been effective in reducing endpoints, there was no placebo control.
ALLHAT: Interventions1
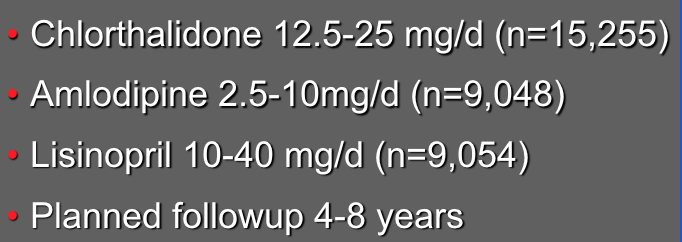
An interim analysis of the ALLHAT population found that the doxazosin arm of the trial substantially lagged behind the other 3 drugs, to the point that there appeared to be no possibility that alpha-blocker outcomes could approach that of the other 3 arms, and it was then discontinued.
The Results
When asked who won the ALLHAT trial, the most commonplace answer is the diuretic. But let’s look a little closer.
Grandma’s health advocate, her granddaughter Geraldine, has asked a very pertinent question: if I’m going to have to convince Grandma that she has to take this medicine—and she is NOT one to usually embrace the healthcare system—is there one medication that has any mortality advantage over another?
While the ALLHAT trial outcomes did show that for specific endpoints, chlorthalidone had advantage over the other 2 agents, for the endpoint of mortality, all 3 drugs were the same.
ALLHAT: Results1

This lends credence to the concept, endorsed by many hypertension experts, that it is more important to get the BP down than which agent you choose to accomplish that.
Some clinicians feel confounded when there is no clear “winner” in a drug comparison trial. On the other hand, this gives us multiple opportunities. For instance, let’s say that you were to institute an ACE inhibitor as the initial choice. If the patient develops a cough and wants to discontinue the ACE, should you be concerned that the next drug choice is “second best”? Not at all, because even though chlorthalidone outperformed the ACE and CCB for specific individual endpoints within ALLHAT, for the endpoint of mortality the outcomes were the same for all 3 agents.
The decision on which drug to use should emerge from issues about patient preference, cost, and adverse effects.
What’s the “Take Home”?
The ALLHAT trial was the largest hypertension trial ever performed (originally ±44,000, reduced to ±33,000 with the elimination of the alpha blocker arm). While it is true that chlorthalidone outperformed ACE and CCB in some specific endpoints, for the endpoint of mortality, all 3 drugs were equally efficacious.
Reference:
1. ALLHAT Group. Major outcomes in high-risk HTN patients randomized to ACEI or CCB vs. diuretic. JAMA. 2002;288:2981-2997