
Peer Reviewed
Therapeutic Choices in Sleep Apnea: Tailoring Treatment to the Patient
Authors:
Adam J. Sorscher, MD
Associate Professor, Community and Family Medicine, Dartmouth-Hitchcock Medical Center, Lebanon, New Hampshire; Medical Director, The Sleep Health Center, Alice Peck Day Memorial Hospital, Lebanon, New Hampshire
Deepa Burman, MD
Associate Professor of Pediatrics, University of Pittsburgh School of Medicine, Pittsburgh, Pennsylvania; Medical Codirector, Pediatric Sleep Program, University of Pittsburgh Medical Center (UPMC) Children’s Hospital of Pittsburgh, Pittsburgh, Pennsylvania; and Medical Director, Portable Sleep Study Program, UPMC McKeesport Hospital, McKeesport, Pennsylvania.
Citation:
Sorscher AJ, Burman D. Therapeutic choices in sleep apnea: tailoring treatment to the patient. Consultant. 2018;58(11):293-305.
ABSTRACT: Obstructive sleep apnea syndrome (OSAS) is a prevalent condition that can diminish the restorative quality of sleep and that has deleterious metabolic and cardiovascular consequences. It is often comorbid with other chronic conditions including diabetes, obesity, and depression. The prevalence of OSAS in adults is estimated to be 3% to 7%, and despite increased awareness and testing in the past 15 years, approximately 80% of cases remain undiagnosed. Helping patients to receive effective treatment remains a challenge: 40% of people with OSAS do not successfully use the treatment of choice, continuous positive airway pressure (CPAP), in the long term. For people who are nonadherent with CPAP, lifestyle modification (weight loss, reducing alcohol intake, and enforced lateral sleep position), dental appliances, and otolaryngology procedures may be sufficiently efficacious and more tolerable in cases of mild to moderate OSAS. For people with severe OSAS who do not tolerate fixed CPAP pressure, use of alternative modes of noninvasive pressure support, such as autotitrate or bilevel, may increase adherence. This article provides a brief discussion of the evaluation of obstructive sleep apnea, a description of strategies to improve CPAP adherence, and a review of alternative therapies for adults who cannot tolerate CPAP.
Obstructive sleep apnea (OSA), first characterized in 1965,1 is marked by repetitive total closures (apneas) or near total closures (hypopneas) of the airway when asleep. These occurrences lead to episodes of ineffective breathing and oxygen desaturation that terminate in brief arousals and resumption of effective breathing.
OSA is rare in the animal kingdom. Humans are the only primates that exhibit it, and its occurrence is due to the fact that the pharynx and hypopharynx participate in 3 significant functions: phonation, respiration, and deglutition. To achieve this versatility, especially human phonation capabilities, the human pharynx has sacrificed bony rigidity and is more collapsible than in other species, especially in the sleep state. Humans also sleep more on their backs than other animal species, contributing to more posterior displacement of the tongue and soft palate into the airway when asleep.
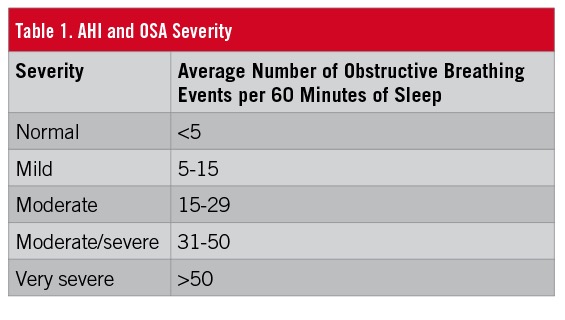
Key risk factors for OSA are obesity, male gender, and advancing age.2 The incidence of OSA has increased dramatically, not only as a result of increased awareness and testing, but also due to the obesity epidemic. The true prevalence of OSA is a subject of debate and depends upon disease definitions. The apnea-hypopnea index (AHI), measured in a sleep study, is a tally of obstructive breathing events averaged per 60 minutes of sleep (Table 1). Using AHI definitions, the prevalence of OSA in the United States is 12%, and it is estimated that 80% of cases remain undiagnosed. The prevalence of OSA syndrome (OSAS), meaning an AHI greater than 5 with symptoms of excessive daytime sleepiness, is reportedly 3% to 7% of the adult population.2
Consequences of OSA
The chief consequences of OSA are snoring, sleep fragmentation, and metabolic stress. Almost all people with OSA exhibit significant snoring. Although most authorities believe that snoring in the absence of apneas and hypopneas does not have direct health consequences, it certainly can aggravate bed partners and worsen their quality of sleep.3
Sleep fragmentation, due to repetitive brief arousals to reestablish breathing, occurs dozens to hundreds of times per night in OSA and is responsible for its association with excessive daytime sleepiness. However, there appears to be significant inter-individual variability in the expression of daytime sleepiness. One study found that only 45% of people with moderate to severe OSA reported hypersomnolence.4 The fact that many people have OSA without overt sleepiness may be part of the reason for why so many cases remain undiagnosed.
Accumulating data point to metabolic stresses caused by OSA. Regarding cardiovascular health, OSA is associated with hypertension, congestive heart failure, coronary artery disease, and arrhythmias.5,6 Other associations have been reported between OSA and weight gain and glucose intolerance.7-9 At present, data are mixed about the success of treatment in reversing cardiovascular endpoints such as myocardial infarction, cerebrovascular accident, and mortality.10
Office Evaluation of OSA
Elements of a patient’s medical history that confer increased risk of comorbid OSA are congestive heart failure, atrial fibrillation, hypertension, diabetes, stroke, pulmonary hypertension, and coronary artery disease.11 A history of loud snoring and witnessed apneas (if there is a bed partner) are important elements of the history of present illness. Regarding physical examination, data from the landmark Sleep Heart Health Study indicate that neck circumference of greater than 43 cm in men and greater than 41 cm in women is a highly predictive indicator of OSA.12,13 Obesity (body mass index [BMI] >30 kg/m2) and retrognathia (suggesting a small airway) are also suggestive features.14
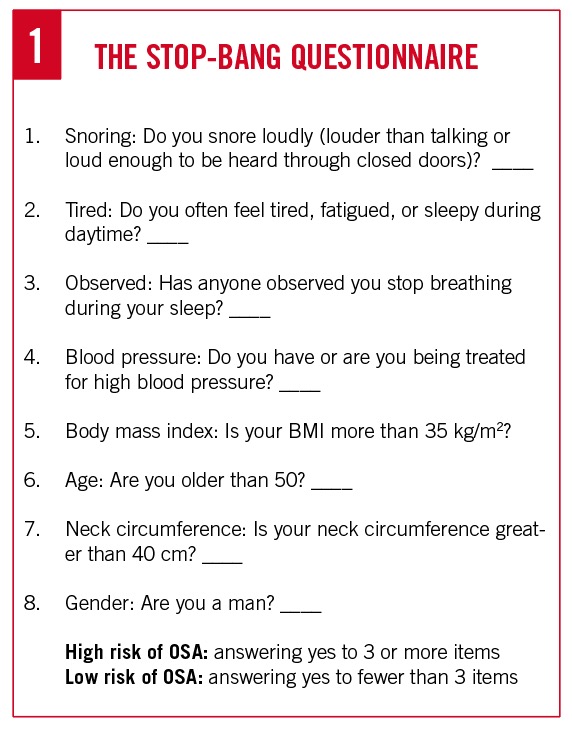
These signs and symptoms are incorporated into screening instruments such as the STOP-Bang Questionnaire (Figure 1). Many physicians’ offices routinely employ the Epworth Sleepiness Scale to gauge hypersomnolence. However, sleepiness per se is neither a specific indicator (since there are many other causes of sleepiness, especially sleep deprivation) nor a sensitive indicator (since many people with OSA are not demonstrably sleepy) of the presence of OSA.
Testing for OSA
Until recently, testing for OSA has been exclusively the province of sleep medicine specialists conducting tests in sleep laboratories. The traditional polysomnogram typically records 17 variables, including electroencephalography/electrooculography/chin tone (together, these are used to establish sleep stage); 2 airflow sensors/abdominal and thoracic gauges (to sense respiratory effort)/continuous oximeter (to detect respiratory pathology), single lead electrocardiography, and leg leads (to record abnormal movements).
The billable cost for a single-night polysomnography study ranges from $1500 to $3000. Beginning in 2008, the Centers for Medicare and Medicaid Services approved reimbursement for home sleep test (HST) devices. These are focused on breathing parameters, usually employing 4 to 7 sensors to track airflow, oximetry, pulse, and sometimes body position but not sleep stages and body movements.
With the emergence of low-cost HSTs, many predicted the demise of laboratory sleep testing. While market share for HSTs has risen slowly, a strong role still exists for testing in the sleep laboratory. Contraindications to HSTs are conditions in which there may be comorbid hypoventilation, hypoxia, and central sleep apnea. These include significant neuromuscular disorders, severe respiratory disease, congestive heart failure, and chronic opioid use. In addition, HST technology has not been well validated in pediatric and elderly populations, and its use is therefore limited to people aged 18 to 65 years.
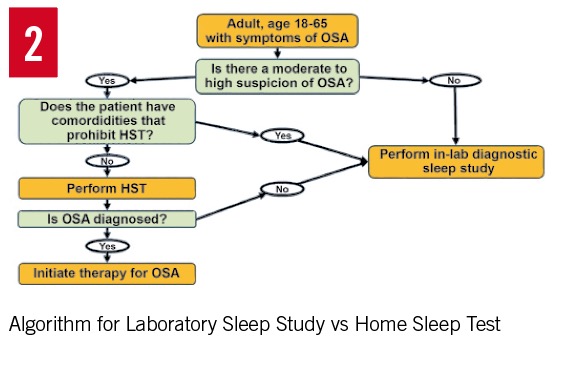
Home sleep tests are best thought of as an inexpensive confirmatory test for OSA in patients with a moderate to high risk of OSA based on symptoms. HST devices invariably underestimate the degree of obstructive breathing events, because they do not detect subtle events marked by airflow attenuation and central nervous system (CNS) arousals but without significant oxygen desaturation. Consequently, most testing algorithms designate a normal HST result as “inconclusive” and recommend that it be followed up with a laboratory-based sleep study to rule out OSA definitively (Figure 2).
AHI Scores: Arousal-Based vs Medicare Scoring Rules
The AHI is a tally of obstructive events averaged per 60 minutes of sleep time and is the usual measure of OSA severity. Apneas and hypopneas are given equal weight in this scoring system because they are both terminated by CNS arousals that produce deleterious sleep fragmentation.
To complicate matters, the report of a sleep study typically includes 2 AHI scores—one using arousal-based criteria and the other using Medicare criteria. In both systems, apneas are defined as a 90% reduction in airflow lasting for 10 seconds. But they differ in their definition of hypopneas. In the arousal-based rules, hypopneas are events marked by reduction in airflow amplitude accompanied by either a 3% desaturation or a CNS arousal, whereas the Medicare rules only count hypopneas with 4% or greater desaturations—a higher threshold. This discrepancy can sometimes lead to significant differences in AHI scores depending on which rules are used.
The controversy that has given rise to these competing definitions of hypopneas arises from the fact that landmark studies linking OSA to negative cardiovascular outcomes have usually used the Medicare 4% desaturation rule to define hypopneas.13 This definition was later adopted by Medicare. In contrast, the arousal-based scoring rules align more closely with sleep fragmentation and attendant daytime sleepiness. From an evidence-based standpoint, a normal Medicare AHI implies that cardiovascular health is not imperiled; a normal arousal-based AHI implies that sleep continuity is not significantly ruined.
One occasional consequence of having 2 competing rules for AHI scoring is that patients might test positive for OSA based on the arousal-based scoring method and negative for OSA using the Medicare rules. Such patients, if older and insured by Medicare, may fail to qualify for insurance coverage for a trial of continuous positive airway pressure (CPAP) therapy.
Treatment of OSA
After OSA has been diagnosed and its severity determined, the treating physician should share the results with the patient and provide education about the risk factors, natural history, and consequences of OSA.
All patients should be counseled to avoid activities that require vigilance and alertness if sleepy. Specifically, they should be warned about the increased risk of motor vehicle accidents associated with untreated OSA and be advised to pull over and take a nap if drowsy when driving.
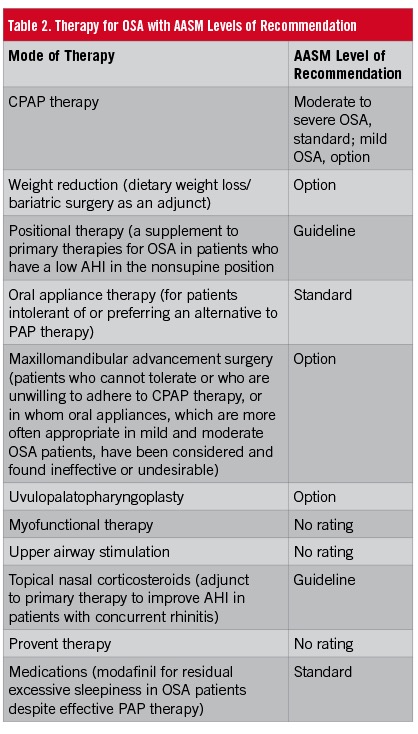
Successful treatment of OSA has been shown to reduce hypertension, levels of daytime sleepiness, motor vehicle accidents, and recurrence of atrial fibrillation after cardioversion, and to improve quality of life measures.15,16 The therapeutic options for OSA are described below, along with evidence-based levels of recommendation by the American Academy of Sleep Medicine (AASM) (Table 2)
CPAP
CPAP therapy, which creates a pneumatic splint that maintains airway patency during sleep, has been the mainstay of management of OSA in adults since 1981.17
CPAP is the most effective therapeutic option, almost always lowering the AHI into the normal range. Consequently, it is the treatment of choice, especially for moderate to severe OSA.18
Improving CPAP Adherence
Most insurers, including Medicare, require evidence of adherence to CPAP therapy in order to provide continuing coverage beyond an initial 12-week trial period. Adequate adherence is usually defined as more than 4 hours of use on 70% of nights (usage is tracked internally by the CPAP machine). Despite many improvements in mask and machine design, adherence to CPAP therapy remains a major challenge—successful long-term adherence is reported to be 65% to 80%.19,20
It is important for physicians to set proper expectations about CPAP therapy—for example, that it might take several weeks to get used to the machine, and that the response to therapy in terms of improved energy and alertness in the daytime is somewhat unpredictable. Comprehensive programs of education about the harms of untreated OSA, CPAP help lines, and group education have improved adherence in some studies.20-22
One key to long-term adherence appears to be close follow-up of patients within the first few weeks of initiating therapy to address tolerability problems. Many sleep medicine programs use clinical sleep educators for this purpose. In addition, CPAP devices have comfort features that also improve adherence, and patients need to be adept at using them, which include the following: a ramp allowing pressure to gradually build at a preset level over a set time; a pressure relief function, resulting in a small drop in pressure during exhalation; heated humidification; and mask liners to decrease air leaks and improve fit.
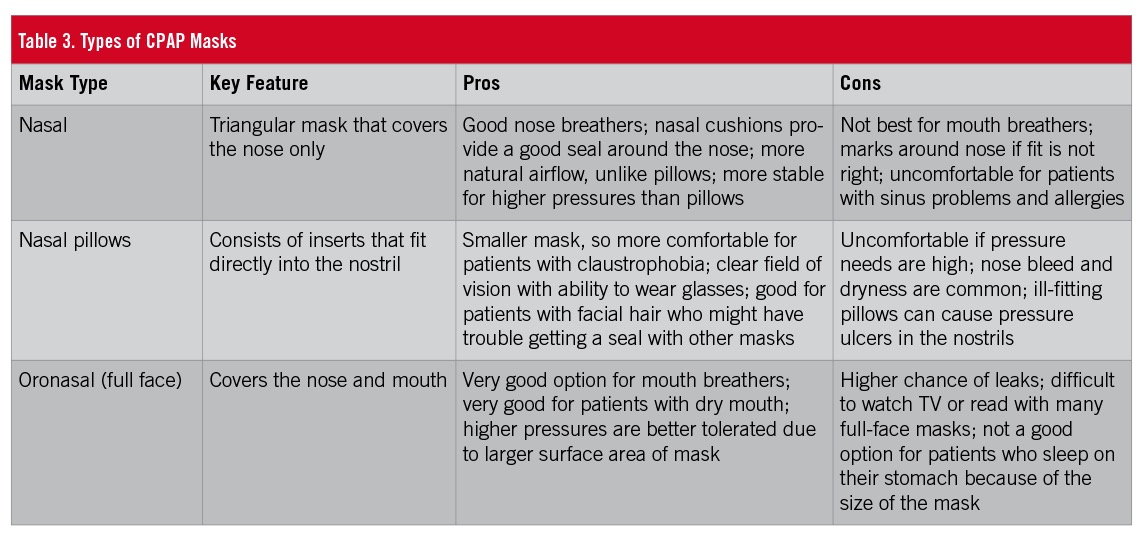
Perhaps the most important modification to improve adherence is finding the right mask interface (Table 3). Patients should be counseled that all masks are equally effective (since the therapy is the pressurized air, not the mask). Patients are usually permitted, during the initial trial period, to try different masks until they find one that is comfortable. When patients use the bathroom in the middle of the night, they should disconnect the hose from the mask and keep their mask on.
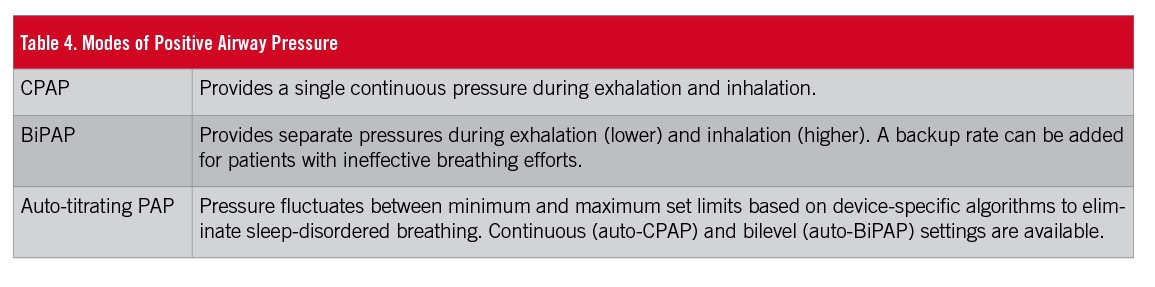
For patients who struggle with excessive force of air or experience aerophagia, switching to other PAP modes may be more tolerable. These include auto-titrating PAP, in which the machine senses airway collapse and adjusts the pressure throughout the night to meet the patient’s need, and bilevel PAP (BiPAP), in which the machine is set to deliver one pressure during inhalation and then a lower pressure during exhalation (Table 4). These settings are usually prescribed by the treating sleep medicine physician in the hope that a different mode may improve adherence. As a compromise, it may be reasonable in some cases to decrease the pressure setting to a level that does not fully prevent all obstruction if it is necessary to improve adherence.
 Alternatives to PAP Therapy
Alternatives to PAP Therapy
While CPAP is the most effective therapy for OSA, reasonably effective alternatives exist for patients who struggle to use it.23 The chief options include lifestyle modification (weight loss, alcohol reduction), positional therapy (emphasize lateral sleep), oral appliances, otorhinolaryngology therapies (surgery, upper airway stimulation, rhinitis therapy), and Provent therapy.
Lifestyle Modifications
Lifestyle modifications such as weight reduction, abstinence from alcohol, and avoiding sedatives/medications with muscle-relaxant properties can mitigate OSA.24
Obesity is present in more than 70% of patients with OSA. Increased BMI is closely correlated with AHI.2 In one study, a 10% reduction in body weight was associated with a 26% to 32% reduction in AHI.25 It is reasonable to reevaluate the degree of OSA if a patient loses 10% of his or her weight.25,26
Weight reduction, whether by intensive lifestyle or pharmacologic intervention or bariatric surgery, is effective in reducing sleep apnea severity. In patients with a BMI of more than 40 kg/m2, bariatric surgery should be considered when conservative treatments have failed.27 Compared with bariatric surgery, nonsurgical weight loss offers lesser improvements in BMI and AHI. Bariatric surgery has resulted in an improvement in AHI in more than 80% of obese patients with OSA and a remission rate of 40% after 2 years.28,29
All patients with OSA should be questioned about their alcohol consumption. Besides potentially contributing to weight gain, alcohol exacerbates OSA by increasing airway collapsibility and by blunting the arousal response to apnea, thereby increasing the duration of obstructive events.30 If there is suspicion of excessive drinking, then mitigation of OSA is one of many reasons to counsel patients to cut down.
Positional Therapy
In many patients, vulnerability to obstructive breathing is strongly linked to supine sleeping position—a form known as positional OSA. Enforced lateral sleeping position can be used in these patients for treatment of sleep apnea. Different techniques to prevent patients from assuming the supine position include positional alarms, verbal instructions, sewing tennis balls into the back of the pajama top, vests, “shark fins,” or special pillows.31
A recent systematic review and meta-analysis including 3 prospective cohort studies and 4 randomized controlled trials revealed that newer devices for positional therapy are effective in reducing AHI during short-term follow-up.32 Combined data show a mean difference of 11.3 events/hour (54% reduction) in AHI and 33.6% (84% reduction) in percentage total sleeping time in the supine position.31,32 These devices are easy to use and reversible. Under study conditions, adherence was found to be very high. Nevertheless, long-term adherence studies of positional therapy are needed to confirm its role as a single or combination treatment modality for patients with OSA.
Oral Appliance Therapy
Oral appliances have emerged as a useful alternative to PAP therapy for treatment of OSA. They improve upper airway obstruction and prevent collapse by changing jaw and tongue position. The 2 main types of oral appliances are tongue retaining and mandibular advancement devices (MADs). MADs, inserted into the oral cavity, push the mandible forward subtly and thereby reduce snoring and OSA.33,34 A candidate for a MAD should first be evaluated by an experienced dentist (preferably certified by American Board of Dental Sleep Medicine) to determine whether it is a feasible and safe treatment from a dental standpoint. Patients must have at least 6 to 10 healthy teeth in both upper and lower arches to insert the device, and they must be able to voluntarily protrude the mandible in order to use a MAD.35 Mild temporomandibular joint (TMJ) dysfunction sometimes improves with MAD use, but moderate to severe TMJ disease and inadequate protrusive ability are considered contraindications to this therapy. MADs can also impact favorably on bruxism because they function as a nightguard and protect the teeth from wearing down.
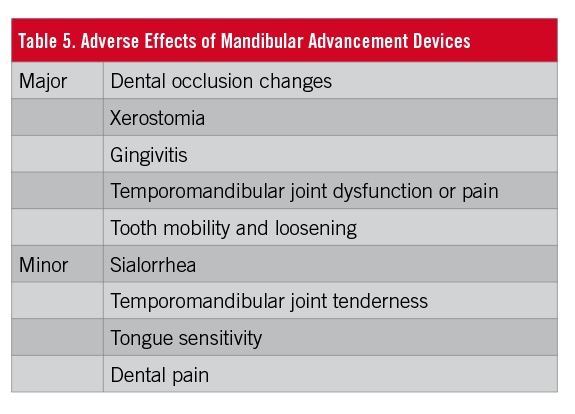
MADs reduce AHI to less than 10 in approximately 50% of patients with mild to moderate OSA.34,36 They are typically less effective than CPAP in terms of absolute AHI reduction, but their positive effects on quality of life and subjective sleepiness are comparable with those of CPAP, perhaps due to better adherence. The AASM recommends MADs for mild to moderate OSA.27 Despite this recommendation and improved adherence rates compared with CPAP, MADs are now used in only 10% of patients treated for OSA. Although the Centers for Medicare and Medicaid Services provides coverage for this option when custom-made by a dentist, coverage by private insurers remains variable. Some reported adverse effects of MADs are presented in Table 5
Tongue-retaining devices, which splint the tongue in place to keep the airway open, have insufficient evidence regarding effectiveness, and they are not used commonly.37
Otorhinolaryngology Surgery
Patients who are unable to tolerate CPAP and who are not candidates for MADs may seek surgical alternatives. The most common simple procedures are the uvulopalatopharyngoplasty (UPPP) in which tonsils and the uvula are removed to create a larger oropharyngeal airway and laser-assisted uvuloplasty. There is insufficient evidence to support either of these procedures, in part due to a lack of data on outcomes such as quality of life and cardiovascular benefits. UPPP specifically is not effective in normalizing AHI in moderate to severe OSA.27
Tracheostomy was the original treatment option for OSA, before the advent of CPAP. Because it bypasses the upper airway entirely, it is perfectly effective. However, because of the aggressiveness of this procedure, it should be considered only when all other options have failed. Other surgical options include multilevel surgery, maxillomandibular advancement, genioglossus (tongue muscle) advancement, and nasal reconstruction surgeries.38
Myofunctional Therapy
Dilator muscles of the upper airway play a critical role in maintaining an open airway during sleep. Several recent studies have investigated the effects of oropharyngeal exercises on OSA severity. One study randomized 31 patients with moderate OSA either to a sham therapy or to a set of oropharyngeal exercises derived from speech therapy. The exercises consisted of isometric and isotonic exercises involving the tongue, soft palate, and lateral pharyngeal wall. Three months of exercise training requiring 24 minutes per day reduced OSA severity by 39%, evaluated by the AHI and lowest oxygen saturation determined by polysomnography.39 A systematic review and meta-analysis of 9 studies of myofunctional therapy for OSA showed an average 50% reduction in AHI. The mechanism by which exercises when awake influence the behavior of upper airway during sleep are not fully understood. In most protocols, the patient must perform these exercises 2 or 3 times a day, and this may limit the clinical application.40
Upper Airway Stimulation
The onset of an apneic episode is marked by reduced activity of nerves that promote airway patency, especially the genioglossus nerve.41
Surgical implantation of an upper-airway neurostimulator has recently been studied by otolaryngologists at 22 academic and private centers. The results showed that unilateral stimulation of the hypoglossal nerve, synchronous with ventilation, resulted in clinically meaningful reductions in the severity of OSA along with self-reported sleepiness, and improvements in quality-of-life measures at 1 year. This technique has shown promise for selected patients in feasibility trials.42
Management of Rhinitis
Rhinitis is only a minor contributor to OSA, since the collapsing events of OSA occur in the pharynx and hypopharynx, not the nasopharynx. However, there is low-quality evidence that short-term intranasal corticosteroids improve the AHI mildly by reducing negative pressure distal to the nasopharynx. This therapy does not improve oxygen saturation, sleep quality, or total sleep time. Topical nasal corticosteroids can be used as an adjunct to treat concomitant rhinitis in OSA patients (and in this context, they may help with CPAP tolerability) and for nonapneic snoring.43
Provent Therapy
Provent consists of disposable 1-way resister valves that are placed over the nostrils with adhesive tape. Patients exhale against high resistance, creating a positive end expiratory pressure that is transmitted to the pharynx. Provent is marketed as a treatment of very mild OSA.44 It might be handy for travelers who do not wish to bring their CPAP device along on a trip. Provent is a single nightly device that is not presently covered by insurers.
Summary
CPAP is the gold standard of treatment for OSA because of its unmatched effectiveness and lack of significant adverse effects, and is the treatment of choice for people with moderate to severe OSA. Close follow-up in the first few weeks of a CPAP trial has been shown to improve adherence, although family medicine offices often lack the infrastructure to provide this support. For patients with mild to moderate OSA or who are unable to tolerate CPAP, there are other reasonable therapeutic alternatives. MADs, custom fit by certified dentists, are an underutilized yet often effective option. No single treatment is best suited for all patients, and successful management of sleep apnea should incorporate various treatment modalities tailored to the needs of the individual patient.
- Jung R, Kuhlo W. Neurophysiological studies of abnormal night sleep and the Pickwickian syndrome. Prog Brain Res. 1965;18:140-159.
- Punjabi NM. The epidemiology of adult obstructive sleep apnea. Proc Am Thorac Soc. 2008;5(2):136-143.
- Beninati W, Harris CD, Herold DL, Shepard JW Jr. The effect of snoring and obstructive sleep apnea on the sleep quality of bed partners. Mayo Clin Proc. 1999;74(10):955-958.
- Kapur VK, Baldwin CM, Resnick HE, Gottlieb DJ, Nieto FJ. Sleepiness in patients with moderate to severe sleep-disordered breathing. Sleep. 2005;28(4):472-477.
- Nieto FJ, Young TB, Lind BK, et al; Sleep Heart Health Study. Association of sleep-disordered breathing, sleep apnea, and hypertension in a large community-based study. JAMA. 2000;283(14):1829-1836.
- Dempsey JA, Veasey SC, Morgan BJ, O’Donnell CP. Pathophysiology of sleep apnea. Physiol Rev. 2010;90(1):47-112.
- Teramoto S, Yamamoto H, Yamaguchi Y, Namba R, Ouchi Y. Obstructive sleep apnea causes systemic inflammation and metabolic syndrome. Chest. 2005;127(3):1074-1075.
- Gami AS, Somers VK. Obstructive sleep apnoea, metabolic syndrome, and cardiovascular outcomes. Eur Heart J. 2004;25(9):709-711.
- Tasali E, Van Cauter E. Sleep-disordered breathing and the current epidemic of obesity: consequence or contributing factor? Am J Respir Crit Care Med. 2002;165(5):562-563.
- Yu J, Zhou Z, McEvoy RD, et al. Association of positive airway pressure with cardiovascular events and death in adults with sleep apnea: a systematic review and meta-analysis. JAMA. 2017;318(2):156-166.
- Aurora RN, Collop NA, Jacobowitz O, Thomas SM, Quan SF, Aronsky AJ. Quality measures for the care of adult patients with obstructive sleep apnea. J Clin Sleep Med. 2015;11(3):357-383.
- Caffo B, Diener-West M, Punjabi NM, Samet J. A novel approach to prediction of mild obstructive sleep disordered breathing in a population-based sample: the Sleep Heart Health Study. Sleep. 2010;33(12):1641-1648.
- Quan SF, Howard BV, Iber C, et al. The Sleep Heart Health Study: design, rationale, and methods. Sleep. 1997;20(12):1077-1085.
- Myers KA, Mrkobrada M, Simel DL. Does this patient have obstructive sleep apnea? The Rational Clinical Examination systematic review. JAMA. 2013;310(7):731-741.
- Campos-Rodriguez F, Queipo-Corona C, Carmona-Bernal C, et al; Spanish Sleep Network. Continuous positive airway pressure improves quality of life in women with obstructive sleep apnea: a randomized controlled trial. Am J Respir Crit Care Med. 2016;194(10):1286-1294.
- Lamberts M, Nielsen OW, Lip GYH, et al. Cardiovascular risk in patients with sleep apnoea with or without continuous positive airway pressure therapy: follow-up of 4.5 million Danish adults. J Intern Med. 2014;276(6):659-666.
- Sullivan CE, Issa FG, Berthon-Jones M, Eves L. Reversal of obstructive sleep apnoea by continuous positive airway pressure applied through the nares. Lancet. 1981;1(8225):862-865.
- Kapur VK, Auckley DH, Chowdhuri S, et al. Clinical practice guideline for diagnostic testing for adult obstructive sleep apnea: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2017;13(3):479-504.
- Weaver TE, Sawyer AM. Adherence to continuous positive airway pressure treatment for obstructive sleep apnoea: implications for future interventions. Indian J Med Res. 2010;131:245-258.
- Delanote I, Borzée P, Belge C, Buyse B, Testelmans D. Adherence to CPAP therapy: comparing the effect of three educational approaches in patients with obstructive sleep apnoea. Clin Respir J. 2018;12(1):91-96.
- Richards D, Bartlett DJ, Wong K, Malouff J, Grunstein RR. Increased adherence to CPAP with a group cognitive behavioral treatment intervention: a randomized trial. Sleep. 2007;30(5):635-640.
- Wozniak DR, Lasserson TJ, Smith I. Educational, supportive and behavioural interventions to improve usage of continuous positive airway pressure machines in adults with obstructive sleep apnoea. Cochrane Database Syst Rev. 2014;(1):CD007736. doi:10.1002/14651858.CD007736.pub2.
- Lorenzi-Filho G, Almeida FR, Strollo PJ. Treating OSA: current and emerging therapies beyond CPAP. Respirology. 2017;22(8):1500-1507.
- Araghi MH, Chen Y-F, Jagielski A, et al. Effectiveness of lifestyle interventions on obstructive sleep apnea (OSA): systematic review and meta-analysis. Sleep. 2013;36(10):1553-1562.
- Cowan DC, Livingston E. Obstructive sleep apnoea syndrome and weight loss: review. Sleep Disord. 2012;2012:163296.
- Tuomilehto H, Seppä J, Uusitupa M. Obesity and obstructive sleep apnea—clinical significance of weight loss. Sleep Med Rev. 2013;17(5):321-329.
- Ramar K, Dort LC, Katz SG, et al. Clinical practice guideline for the treatment of obstructive sleep apnea and snoring with oral appliance therapy: an update for 2015. J Clin Sleep Med. 2015;11(7):773-8
- Sarkhosh K, Switzer NJ, El-Hadi M, Birch DW, Shi X, Karmali S. The impact of bariatric surgery on obstructive sleep apnea: a systematic review. Obes Surg. 2013;23(3):414-423.
- Romero-Corral A, Caples SM, Lopez-Jimenez F, Somers VK. Interactions between obesity and obstructive sleep apnea: implications for treatment. Chest. 2010;137(3):711-719.
- Scanlan MF, Roebuck T, Little PJ, Redman JR, Naughton MT. Effect of moderate alcohol upon obstructive sleep apnoea. Eur Respir J. 2000;16(5):909-913.
- Ravesloot MJL, van Maanen JP, Dun L, de Vries N. The undervalued potential of positional therapy in position-dependent snoring and obstructive sleep apnea—a review of the literature. Sleep Breath. 2013;17(1):39-49.
- Ravesloot MJL, White D, Heinzer R, Oksenberg A, Pépin J-L. Efficacy of the new generation of devices for positional therapy for patients with positional obstructive sleep apnea: a systematic review of the literature and meta-analysis. J Clin Sleep Med. 2017;13(6):813-824.
- Ferguson KA, Cartwright R, Rogers R, Schmidt-Nowara W. Oral appliances for snoring and obstructive sleep apnea: a review. Sleep. 2006;29(2):244-262.
- Sutherland K, Vanderveken OM, Tsuda H, et al. Oral appliance treatment for obstructive sleep apnea: an update. J Clin Sleep Med. 2014;10(2):215-227.
- Bailey DR. Dental therapy for obstructive sleep apnea. Semin Respir Crit Care Med. 2005;26(1):89-95.
- Park P, Jeon HW, Han DH, et al. Therapeutic outcomes of mandibular advancement devices as an initial treatment modality for obstructive sleep apnea. Medicine (Baltimore). 2016;95(46):e5265.
- Deane SA, Cistulli PA, Ng AT, Zeng B, Petocz P, Darendeliler MA. Comparison of mandibular advancement splint and tongue stabilizing device in obstructive sleep apnea: a randomized controlled trial. Sleep. 2009;32(5):648-653.
- Aurora RN, Casey KR, Kristo D, et al. Practice parameters for the surgical modifications of the upper airway for obstructive sleep apnea in adults. Sleep. 2010;33(10):1408-1413.
- Guimarães KC, Drager LF, Genta PR, Marcondes BF, Lorenzi-Filho G. Effects of oropharyngeal exercises on patients with moderate obstructive sleep apnea syndrome. Am J Respir Crit Care Med. 2009;179(10):962-966.
- Camacho M, Certal V, Abdullatif J, et al. Myofunctional therapy to treat obstructive sleep apnea: a systematic review and meta-analysis. Sleep. 2015;38(5):669-675.
- Schwartz AR, Barnes M, Hillman D, et al. Acute upper airway responses to hypoglossal nerve stimulation during sleep in obstructive sleep apnea. Am J Respir Crit Care Med. 2012;185(4):420-426.
- Huntley C, Kaffenberger T, Doghramji K, Soose R, Boon M. Upper airway stimulation for treatment of obstructive sleep apnea: an evaluation and comparison of outcomes at two academic centers. J Clin Sleep Med. 2017;13(9):1075-1079.
- Morgenthaler TI, Kapen S, Lee-Chiong T, et al. Practice parameters for the medical therapy of obstructive sleep apnea. Sleep. 2006;29(8):1031-1035.
- Friedman M, Hwang MS, Yalamanchali S, Pott T, Sidhu M, Joseph NJ. Provent therapy for obstructive sleep apnea: impact of nasal obstruction. Laryngoscope. 2016;126(1):254-259.