
Peer Reviewed
Retropharyngeal Tear
Authors:
Kim Nguyen, MD, and Karen Theoktisto, DNP
University of Florida College of Medicine, Gainesville, Florida
Citation:
Nguyen K, Theoktisto K. Retropharyngeal tear [published online October 18, 2018]. Gastroenterology Consultant.
A previously healthy 2-year-old boy presented with a 2-day history of dysphagia. He refused to eat or drink and would not swallow his saliva and thus was constantly drooling. He also refused to speak. The boy’s mother had noticed that morning that he had been refusing to look up or turn his head and neck to the left or right.
Physical examination. The patient had no stridor, dyspnea, or wheezing. Vital signs were normal, with a weight of 11.8 kg, temperature of 37°C, heart rate of 111 beats/min, respiratory rate of 18 breaths/min, and oxygen saturation of 96% on room air. During the physical examination, the patient resisted moving his head up, even with passive movement, and he followed upward only with his eyes. The uvula was midline, and the tonsils were not enlarged, but there was redness and inflammation of the posterior pharynx. The rest of the physical examination findings were normal.
Diagnostic tests. The patient was sent for a stat soft-tissue neck radiograph, which showed air in the retropharyngeal space with thickened soft tissues, concerning for retropharyngeal abscess (Figure 1). He was sent to the emergency department, where a computed tomography scan was performed, the results of which showed a mucosal tear in the retropharyngeal soft tissues at the C2 level with associated retropharyngeal gas (Figures 2 and 3). He was admitted to the pediatric hospital for further evaluation and management.

Figure 1. Soft-tissue neck radiograph showing air in the retropharyngeal space.
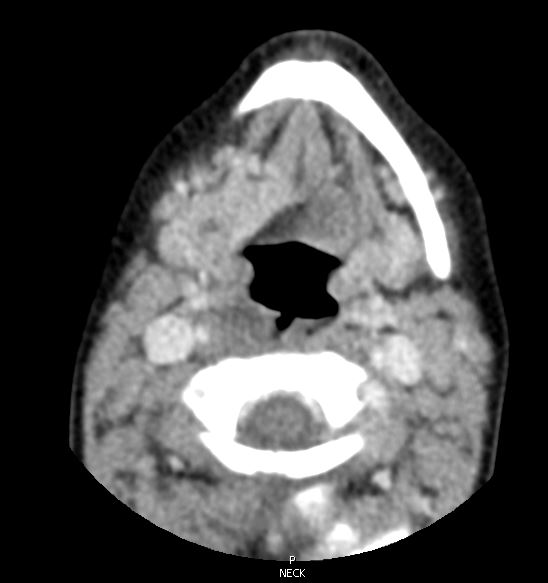
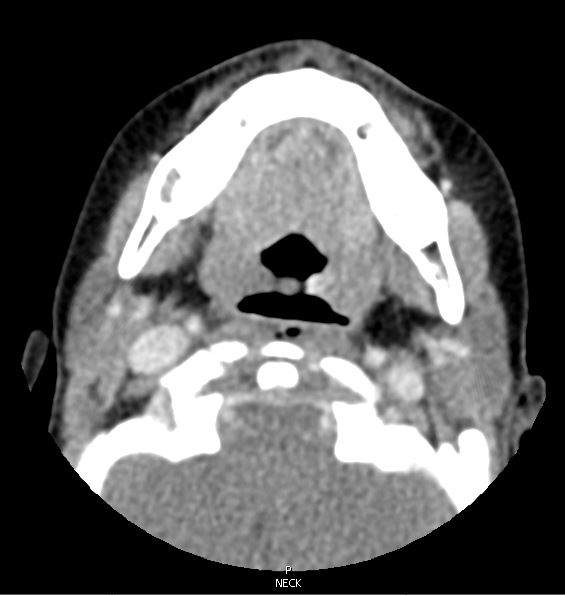
Figures 2 and 3. Computed tomography imaging of the neck showing a mucosal tear at the C2 level with air in the retropharyngeal space.
During further discussion, the boy’s mother stated that he places many inedible objects in his mouth. She recalled that he had been eating candy canes and playing with Nerf foam bullets the night before when the symptoms had started.
Outcome of the case. In the hospital, the patient was placed on intravenous (IV) fluids and IV clindamycin after consultation with a pediatric otorhinolaryngologist. Abdominal radiography results did not reveal any radiopaque objects. He was eventually transitioned to solid foods, which he tolerated well. He was discharged home and made a full recovery.
Discussion. The most common cause of pharyngeal perforation is iatrogenic, such as difficult intubations. There are reports of perforations occurring in neonates in the intensive care unit setting due to endotracheal tube placements, suction catheters, and nasogastric tubes.1,2 Trauma is a less common cause of pharyngeal perforation.
Management consists of either nonoperative or surgical intervention and depends on the size and location of the perforation. In one retrospective study, 11 of 13 pediatric esophageal perforation cases were treated conservatively.3 Conservative, nonoperative management includes intravenous perfusion, analgesics, total parental nutrition, and broad-spectrum antibiotics.
In this 2-year-old, the etiology of the retropharyngeal tear most likely was a traumatic esophageal perforation from a sharp piece of candy. Foreign-body accidents in children younger than 4 years account for 80% of all cases of injury in the retropharyngeal space.4,5 Foreign bodies swallowed or choked on by children can include coins, batteries, pens, sharp candy, bones, and toys. Oral injuries can occur when a child accidently falls down while holding an object such as a toy, stick, or toothbrush in his or her mouth.
The overall mortality associated with pharyngeal perforation is as high as 20%, and a delay in treatment of more than 24 hours after perforation can result in upwards of 40% mortality.6 Pediatric retropharyngeal tear is a rare occurrence that can develop quickly into an abscess. Abscesses in the deep neck space can occur from the perforation trauma but typically are seen in older children and adults. Airway obstruction and abscess that spreads to nearby anatomical structures create the potential for significant morbidity and mortality.
Retropharyngeal perforation secondary to blunt trauma to the posterior pharynx is a rare entity. It is important to keep esophageal trauma due to foreign body perforation in the differential diagnosis when a child presents with dysphagia, stridor, or refusal to eat or drink. These symptoms may suggest an abnormal airway or an internal injury. A timely diagnosis is paramount to avoid potential serious complications.
References:
- Nagaraj HS, Mullen P, Groff DB, Shearer LT, Cook LN. Iatrogenic perforation of the esophagus in premature infants. Surgery. 1979;86(4):583-589.
- Meyers AD, Lillydhal P, Brown G. Hypopharyngeal perforations in neonates. Arch Otolaryngol. 1978;104(1):51-54.
- van der Zee DC, Festen C, Severijnen RS, van der Staak FH. Management of pediatric esophageal perforation. J Thorac Cardiovasc Surg. 1988;95(4):692-695.
- Tomito H, Yamashiro T, Ikeda H, Fujikawa A Kurihara Y, Nakajima Y. Fluid collection in the retropharyngeal space: a wide spectrum of various emergency diseases. Eur J Radiol. 2016;85(7):1247-1256.
- Correa S, Valero JJ, Torres JP, Fierro F. Common carotid perforation secondary to an ingested fish bone in a child: case report. J Pediatr Surg Case Rep. 2016;8:7-9.
- Diep J, Kam D, Kuenzler KA, Arthur JF. Emergent airway management of an uncooperative child with a large retropharyngeal and posterior mediastinal abscess. A A Case Rep. 2016;6(3):61-64.