
Why Does This Young Child Refuse to Walk?
A 25-month-old white female presented with a 1.5-week history of intermittent, cramping, diffuse abdominal pain, increasing irritability, and decreased activity. She has not been running around like she normally does and has been refusing to walk, although she has not been complaining of leg pain.
The child sometimes cries when changing positions on lower half of her body, but reports no pain with using her arms or hands. The parents noticed her gait is a little bit wobbly, but there is no history of falls or trauma.
The parents deny any fever, vomiting, diarrhea, headache, rash, bruising, and flank or back pain. Her appetite has been slightly decreased.
History
The child was seen at an outside hospital 2 days ago where a urinalysis and kidney, ureter, bladder (KUB) x-ray were performed, both of which were negative. She was diagnosed with constipation and treated with a glycerine suppository. She had a bowel movement at home after being discharged, but did not feel better.
The parents reported that the girl had cold symptoms 3 weeks prior, which spontaneously disappeared after several days. Her past medical history was significant for a prior gluteal skin abscess due to methicillin-resistant Staphylococcus aureus (MRSA), which required incision and drainage several months ago.
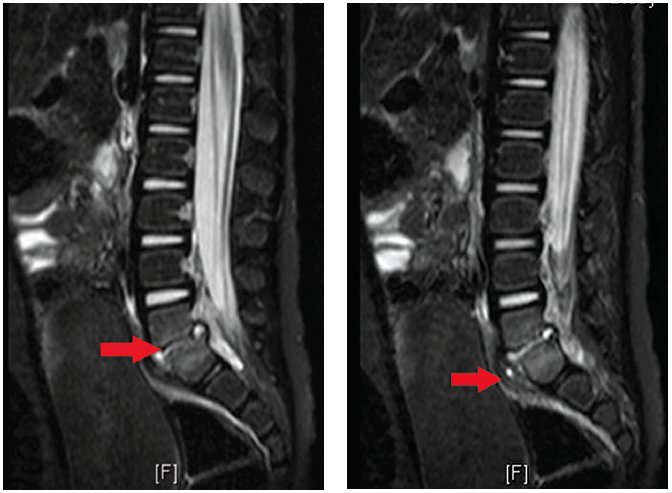
Figure 1. Decreased disc space with bony erosions of the endplates of L5-S1 (arrow).
Figure 2. Perivertebral soft tissue swelling, consistent with a phlegmon (arrow).
Physical Examination
The patient was afebrile with stable vital signs. She was sitting on her mom’s lap and did not want to walk. When she finally took a few steps, her gait was wide-based and waddling, but symmetric and without limping. She had a hyperlordotic stance.
The rest of her exam—including abdominal, genital, neurological, lower extremity, spine, and skin—was normal.
Laboratory Tests
Laboratory results show a white blood cell count of 11.500/µL, with 56% segmented neutrophils and 531.000 platelets, an elevated C-reactive protein (CRP) of 3.9 mmol/L and erythrocyte sedimentation rate (ESR) of 69 mm/hr, and normal creatinine kinase and urinalysis. The KUB study showed mild constipation.
What's Your Diagnosis?
A. Constipation
B. Perirectal absces
C. Transient synovitis of bilateral hips
D. Discitis
(Answer and discussion on next page)
Answer: Discitis
The MRI of the spine (Figure 1) demonstrated an abnormal signal intensity in the lower aspect of L5 and the upper aspect of the S1 vertebral body, which was irregular and had erosion of the endplates. An abnormal signal intensity in the L5-S1 disc space with prevertebral soft tissue swelling was suggestive of phlegmon (Figure 2). A small fluid collection suggestive of an abscess was seen in the prevertebral space, measuring approximately 3 mm x 6 mm.
There was some abnormal signal intensity in the epidural space posterior to L5-S1 level, which was suggestive of a phlegmon. There was a small amount of fluid posterior to the L5-S1 disc space measuring approximately 2 mm x 3 mm, which likely represented a tiny abscess.
Finally, there was enhancement of the phlegmon on the postcontrast T1 images.
The patient underwent a CT guided biopsy with washout, but the cultures did not grow any organisms.
Discussion
Vertebral discitis occurs mostly in patients over 50 years old. Pathogens can reach the bones of the spine by 3 basic routes: hematogenous spread from a distant focus of infection, direct inoculation from trauma or spinal surgery, or contiguous spread from an adjacent soft tissue infection.
The most important infecting organism is S. aureus, accounting for more than 50% of cases. As the proportion of S. aureus strains that are methicillin-resistant has increased during the past decade, the relative importance of MRSA as a cause of vertebral osteomyelitis has also increased. Less common but important pathogens include1,2:
• Enteric gram-negative bacilli, particularly after urinary tract instrumentation
• Pseudomonas aeruginosa and Candida spp. are frequently associated with intravascular access sepsis or injection drug use2
• Groups B and G hemolytic streptococci, especially in patients with diabetes mellitus
• Tuberculosis infection
Clinical Manifestations
The major clinical manifestations of vertebral osteomyelitis include back or neck pain. Spinal pain usually begins insidiously, and progressively worsens over several weeks and sometimes over several months. The pain is often worse at night. Bed rest may help relieve the pain, at least initially.
Patients whose infections extend posteriorly into the epidural space may present with clinical features of an epidural abscess. This often consists of a typical sequence of back pain, which is often local and severe, followed by root pain, motor weakness and sensory changes, and eventually paralysis. Fever is an inconsistent finding.
On physical examination, local tenderness to gentle spinal percussion is the most reliable clinical sign; this is frequently accompanied by reduced back mobility and/or protective spasm of nearby muscles. Rarely, there is a visible mass or even spinal deformity. The physical examination should include palpation for a distended bladder, a check for the signs of psoas abscess (eg, flank pain, limitations of and pain on hip movement), and a careful neurologic assessment of the lower limbs.
Laboratory and Imaging Tests
The leukocyte count may be elevated or normal, but more than 80% of patients have elevations in the ESR, which can exceed 100 mm/hr, and in the acute phase reactant, CRP.3 Blood cultures are positive in up to 50% to 70% of patients with vertebral osteomyelitis.2 They should be obtained in all patients with suspected vertebral osteomyelitis because positive blood cultures may obviate the need for invasive diagnostic tests.
• Bone radiography. Typical findings in vertebral osteomyelitis consist of destructive changes of 2 contiguous vertebral bodies with collapse of the intervening disc space. However, bone destruction may not be apparent for 2 to 3 weeks or more after the onset of symptoms.1
• Computed tomography. CT shows typical or suggestive changes of vertebral osteomyelitis before such changes are apparent on plain films. However, subtle abnormalities detected by CT scanning, such as endplate irregularities, may not be specific for osteomyelitis and early destructive changes may be missed by this imaging technique.
• Magnetic resonance imaging. MRI is the most sensitive radiologic technique to detect vertebral osteomyelitis.4 MRI is also superior to CT scanning for detection of epidural abscesses, but cannot be used in patients with certain metal implants. MRI abnormalities consistent with osteomyelitis can be seen before plain films become abnormal.
• Biopsy. Biopsy is generally needed to confirm the clinical and/or radiographic suspicion of vertebral osteomyelitis. Biopsy material may be obtained via an open procedure or needle biopsy by CT guidance. The samples should be sent for aerobic, anaerobic, mycobacterial, and fungal cultures, and pathology.1
Treatment
Most cases of discitis respond to antimicrobial therapy. However, surgery is necessary in some patients. When the culture and/or Gram stain of the CT-guided needle biopsy is positive, antibiotic therapy should be guided by the results of susceptibility testing. In patients with negative cultures and Gram stains despite repeat biopsies and in unstable patients, empiric antibiotic treatment should be started.
An appropriate regimen consists of vancomycin (15-20 mg/kg every 8-12 hours) plus one of the following: cefotaxime (2 g IV every 6 hours), ceftazidime (1 to 2 g IV every 8-12 hours), ceftriaxone (1 g to 2 g IV daily), cefepine (2 g IV every 12 hours), or ciprofloxacin (400 mg IV every 12 hours or 500 mg to 750 mg orally twice daily).
Treatment should last a minimum of 6 weeks. Longer therapy may be necessary for patients with advanced disease. Surgical debridement is necessary in a minority of patients.
Complications
The most serious complication of vertebral osteomyelitis is neurologic impairment secondary to either abscess formation or bony collapse. Most, but not all, patients have gradual improvement in back pain after therapy is begun, and the pain typically disappears after bone fusion occurs. However, back pain can persist. The best way to reduce the morbidity and mortality associated with vertebral osteomyelitis is to limit the time between the onset of symptoms and the initiation of appropriate therapy.
Differential Diagnosis
• Constipation is common in children. Children with constipation can present with fecal impaction and severe colicky lower abdominal pain. In a series of 83 children presenting to primary care providers or an emergency department with acute abdominal pain, acute or chronic constipation was the most common underlying cause, occurring in 48% of patients. In many cases, rectal examination was a key step in establishing the diagnosis.
Constipation is likely in children with at least 2 of the following characteristics: <3 stools weekly, fecal incontinence (usually related to encopresis), large stools palpable in the rectum or through the abdominal wall, retentive posturing, or painful defecation.5 Parents may not recognize the relationship of constipation to the child’s abdominal pain.
• Perianal abscesses are collections of purulent material that originates from an infected crypt gland in the anus or rectum. Perianal abscesses traverse distally in the intersphincteric groove into the perianal skin, where they present as a tender, fluctuant mass. A perianal abscess, if undrained, can expand into adjacent tissues (eg, ischiorectal or supralevator space). It can also progress to a generalized systemic infection.
Patients with a perianal abscess often present with severe pain in the anal or rectal area. The pain is constant and can be associated with a bowel movement. Constitutional symptoms such as fever and malaise are common. Purulent rectal drainage can be present if the abscess has begun to drain spontaneously.
On physical examination, an area of fluctuance or a patch of erythematous, indurated skin overlying the perianal skin may be noted. However, in some patients and with some types of abscesses (eg, supralevator) there are no findings on physical inspection, and the abscess can only be felt via digital rectal examination.
The diagnosis of a perianal abscess is based upon the findings from the history and physical examination and includes anorectal pain, fever, and a palpable perirectal mass. Imaging studies, such as CT or MRI, are helpful in the setting of a clinical suspicion of nonpalpable anorectal abscess. While anal fistula and perirectal abscess share some features with pilonidal disease, perirectal abscesses are generally near the anus, and anal fistulas generally present as either a perirectal abscess or as a draining pustule in the perianal area or on a buttock.
A perianal abscess can be managed in the office or emergency department using local anesthesia. Complex abscesses should be drained in the operating room.
• Transient synovitis is characterized by pain and limited range of motion in the hip, without clear cause and resolving gradually with conservative therapy. It occurs in children age 3 to 8, with a mean age at presentation of 6 years. The male-to-female ratio is slightly greater than 2:1. Symptoms affect both hips in 5% of children. Cumulative lifetime risk is 3%. Children with transient synovitis generally appear well. Systemic symptoms, including high fever, may occur, but fever typically is absent or low grade.
Septic arthritis of the hip must be excluded. Patients who are nontoxic with minimal fever (temperature <101.3ºF), white blood count <12,000 cells/microL, and ESR <20 mm/hour or CRP <2 mg/dL, often can be followed clinically.6-8 Patients with clinical or laboratory findings of concern should undergo hip ultrasonography. Diagnostic arthrocentesis may be necessary to definitively exclude septic arthritis.
The management of transient synovitis is conservative. Rest, NSAIDs, and return to full activity as tolerated are recommended. The prognosis usually is excellent.
The etiology of transient synovitis is unclear; posttraumatic, allergic, and infectious causes have been proposed.9,10 Between 32% and 50% of children presenting with transient synovitis have had a recent upper respiratory tract infection, therefore an infectious cause is commonly assumed. In a small study of patients with transient synovitis, approximately 50% had elevated blood and/or synovial fluid interferon levels, and approximately 50% had elevated antibody titers to Mycoplasma pneumoniae or a range of viruses (sometimes more than one), including parvovirus B19.9,10 Synovial fluid viral cultures were negative. The significance of these findings is uncertain, because no control patients were tested.
Outcome of the Case
The patient was hospitalized for 12 days and treated with intravenous ceftriaxone and vancomycin, and then treated at home with intravenous clindamycin for 38 days via a peripherally inserted central catheter line. She still has occasional pain at the site and requires ibuprofen 2 to 3 times a week. ■
Maya Myslenski, MD, is assistant professor at Case Western Reserve University and attending physician in the department of emergency medicine at MetroHealth Medical Center in Cleveland, OH.
David Effron, MD, is an assistant professor of emergency medicine at Case Western Reserve University School of Medicine, attending physician in the department of emergency medicine at MetroHealth Medical Center, and consultant emergency physician at the Cleveland Clinic Foundation, all in Cleveland, OH.
References:
1. Lew DP, Waldvogel FA. Osteomyelitis. Lancet. 2004;364(9431):369-379.
2. Nolla JM, Ariza J, Gómez-Vaquero C, et al. Spontaneous pyogenic vertebral osteomyelitis in nondrug users. Semin Arthritis Rheum. 2002;31(4):
271-278.
3. Unkila-Kallio L, Kallio MJ, Eskola J, Peltola H. Serum C-reactive protein, erythrocyte sedimentation rate, and white blood cell count in acute hematogenous osteomyelitis of children. Pediatrics. 1994;93(1):59-62.
4. An HS, Seldomridge JA. Spinal infections: diagnostic tests and imaging studies. Clin Orthop Relat Res. 2006;444:27-33.
5. Loening-Baucke V, Swidninski A. Constipation as a cause of acute abdominal pain in children. J Pediat. 2007;151(6):666-669.
6. Kocher MS, Mandiga R, Zurakowski D, et al. Validation of a clinical prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am. 2004;86-A(8):1629-1635.
7. Caird MS, Flynn JM, Leung YL, et al. Factors distinguishing septic arthritis from transient synovitis of the hip in children. A prospective study. J Bone Joint Surg Am. 2006;88(6):1251-1257.
8. Singhal R, Perry DC, Khan FN, et al. The use of CRP within a clinical prediction algorithm for the differentiation of septic arthritis and transient synovitis in children. J Bone Joint Surg Br. 2011;93(11):1556-1561.
9. Tolat V, Carty H, Klenerman L, Hart CA. Evidence for a viral aetiology of transient synovitis of the hip. J Bone Joint Surg Br. 1993;75(6):973-974.
10. Miron D, Luder A, Horovitz Y, et al. Acute human parvovirus B-19 infection in hospitalized children: A serologic and molecular survey. Pediatr Infect Dis J. 2006;25(10):898-901.