
What Caused This Pregnant Woman’s Abdominal Eruption?
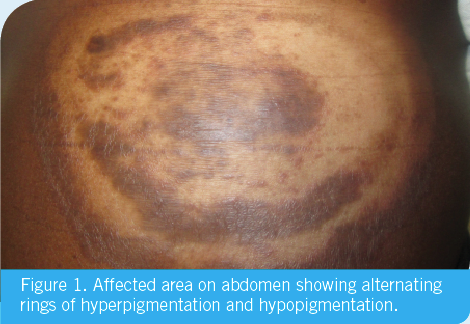
A 23-year-old African American female presented with a 5-month history of a pruritic eruption (Figure 1) confined to the abdomen that developed while she was living in Africa. She was 3 months pregnant at the time of presentation and reported that she had used 0.05% betamethasone lotion prescribed by a family friend as well as 1% hydrocortisone cream obtained over-the-counter without benefit.
Physical Examination
Physical examination revealed concentric erythematous scaling plaques with surrounding hyperpigmentation and hypopigmentation.
Diagnostic and Laboratory Findings
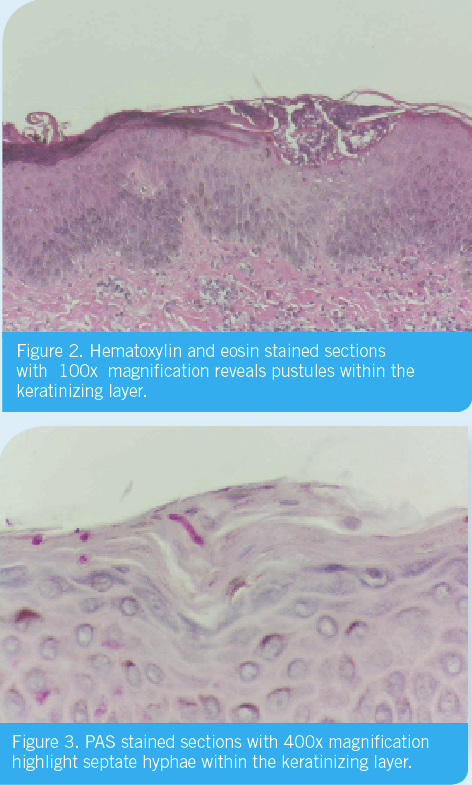
A punch biopsy specimen revealed numerous septate hyphae within the keratinizing layer. (Figures 2 and 3).
Answer and discussion on next page
Answer: Tinea corporis with features of Tinea imbricate
Discussion
Tinea corporis is a dermatophyte infection that most often involves the exposed skin of the trunk and extremities.1 There are more than 40 species of dermatophytes and they are classified into 3 genera: Microsporum, Trichophyton, and Epidermophyton.2 T. rubrum is the most common pathogen, which causes tinea corporis worldwide, but any dermatophyte can be responsible. Transmission can be human-to-human, animal-to-human, or soil-to-human.1,2 Exposure to contaminated surfaces and immunosuppression can also be risk factors. Warmth and humidity are associated with higher frequencies of tinea corporis.2
The typical incubation period is 1 to 3 weeks and the infection spreads centrifugally from the point of original contact. The central clearing results in the clinical appearance of annular lesions.1
Tinea corporis can be expressed as multiple clinical variants, including the inflammatory, perifollicular Majocchi’s granuloma, kerions, tinea profunda with subcutaneous abscess formations, mycetomas, tinea incognito (found when glucocorticosteroid treatment alters the original appearance), and tinea imbricata (with multiple, concentric, and polycyclic lesions).2
Pathogenesis
Because of their ability to metabolize keratin, dermatophytes can live in skin, hair, and nails. A hospitable environment is critical for the dermatophyte to grow. Trauma, increased hydration, maceration, and occlusion can all contribute to the development of tinea.
Dermatophytes produce keratinases and other proteolytic enzymes that play a role in colonization and invasion. The immunologic response of the host is felt to be multifactorial. The presence of a serum inhibitory factor, believed to be an unsaturated transferrin, appears to be important in limiting dermatophyte growth.2 The primary immunologic defense mechanism is type IV delayed hypersensitivity, and after the development of cell-mediated immunity, the infected area is seen to be less inflammatory and eventually involutes.2 Recurring incidences of infection should lead the care provider to check for HIV
infection or diabetes mellitus.3
Histological patterns
As with other dermatophyte infections, tinea corporis is identifiable by a potassium hydroxide preparation that will show septate hyphae and arthrospores in the stratum corneum.2 Furthermore, one may inoculate a sample on Sabouraud dextrose agar and stain the sample with calcofluor and identify Trichophyton by its propensity to fluoresce apple-green under the microscope.1,2
Two stains are useful in the identification of fungi in histological sections: the periodic acid-Schiff stain and the methenamine silver nitrate stain. The former stains fungi a deep red while the latter stains fungi black.4
Differential Diagnosis
Without histological or culture confirmation, tinea may be misdiagnosed as allergic contact dermatitis, atopic dermatitis, annular erythemas, psoriasis, seborrheic dermatitis, pityriasis rosea, pityriasis alba, erythema migrans, subacute lupus erythematosus, or cutaneous T cell lymphoma.5
There have been several reported cases of tinea pseudoimbricata, in which T. tonsurans causes tinea corporis which mimics the annular, concentric rings of tinea imbricata.6-8 The designation as tinea imbricata, however, is reserved to a dermatophyte infection specifically of the T. concentricum strain.1 In such cases, immunosuppression is thought to be an important underlying factor. One such case involved a patient who had recently undergone a renal transplant and subsequently underwent a course of systemic immunosuppressants.8 Treatment with corticosteroids may induce local immunosuppression, which causes the rash to segment into concentric rings.6,7 We believe that this likely explains the striking findings in our case.
Treatment
Topical antifungals provide a good first line of treatment for tinea corporis. Patients who do not respond to topical antifungal therapy should be treated with oral agents such as terbinafine, fluconazole, or itraconazole as long as no contraindications exist.3 Appropriate dosages are as follows: terbinafine 250 mg daily for 1 to 2 weeks, fluconazole 150 mg once weekly for 2 to 4 weeks, and itraconazole 200 mg daily for 1 to 2 weeks.3
Outcome of the Case
Topical terbinafine led to prompt resolution of the skin lesions.
References:
1. Bolognia, J. Dermatology: 3 ed, Vol.2; 2009:1255-1256.
2. Fitzpatrick, T. Dermatology in General Medicine New York: 5 ed, Vol.2. New York; 1999:2346-2348.
Additional references at www.consultant360.com.
3. Ofori, A. Dermatophyte (Tinea) Infections February 2014 Available from: http://www.uptodate.com/contents/dermatophyte-tinea-infections (Accessed March 2014).
4. Elder, D. Lever’s Histopathology of the Skin Philadelphia: 8 ed. Pennsylvania;1997:520-521.
5. Wolff, K. Color Atlas and Synopsis of Clinical Dermatology New York: 7 ed. New York; 2013:618-619.
6. Hoque, S. Trichophyton tonsurans infection mimicking tinea imbricata. 32: Clinical and Experimental Dermatology 2005; 345 - 346.
7. Ouchie, T. Trichophyton Tonsurans Infection Manifesting as Multiple Concentric Erythemas. 32: The Journal of Dermatology 2005; 565 - 568.
8. Lim, S. Tinea pseudoimbricata: Tinea corporis in a renal transplant recipient mimicking the concentric rings of tinea imbricata. (28): Clinical and Experimental Dermatology 2003;332-333.