
Unresolved Acute Pneumonia: a “BAD OMEN”
Authors:
Laren Tan, MD, and Samuel Louie, MD
Citation:
Tan L, Louie S. Unresolved acute pneumonia: a “BAD OMEN.” Consultant. 2017;57(8):500-503.
The most widespread and fatal of all acute infectious diseases, pneumonia, is the “Captain of the Men of Death,” asserted Sir William Osler in the 1901 edition of Principles and Practice of Medicine.1 Pneumonia and influenza were responsible for the largest number deaths from infectious disease in the 20th century.2
Even with the arsenal of antibiotics and vaccines available in the 21st century, community-acquired pneumonia (CAP) has lost none of its virulence. In 2014, pneumonia and influenza together were the leading cause of infectious disease-related death and the eighth leading cause of death overall, with a generalized mortality rate between 15% and 20% in US adults.3
More women than men die from pneumonia and influenza in the United States, but men are 25% more likely than women to die from these diseases, given that there are more women than men in the United States.4 Approximately 85% of all deaths from pneumonia and influenza occur in persons aged 65 years or older.4 More than 1 million hospitalizations due to pneumonia and 7000 due to influenza occurred in 2010 in the United States.4 Death from CAP in the United Kingdom, for example, is reportedly less than 1% among outpatients and 8% to 14% among hospitalized adults and can reach 50% when intensive care unit admission is needed for the management of severe sepsis or acute respiratory failure.5
The most frequent causes of lethal CAP are Streptococcus pneumoniae and Legionella pneumophila.6 The mortality from acute pneumonia has not declined significantly since the introduction of sulfa drugs in the mid-1930s and penicillin in the mid-1940s because of year-to-year variations in influenza virulence and increasing longevity with chronic diseases, including some cancers. The improvement in mortality from infectious diseases has been attributed to better population hygiene, sanitation, and vaccinations.7 The emergence of antibiotic drug resistance in the absence of new antibiotic development and choices threatens to worsen mortality from CAP worldwide.
DIAGNOSIS OF PNEUMONIA
Delay in diagnosis of CAP and further delay in instituting empiric antibiotic treatment and supportive care within 4 hours after diagnosis in a hospital setting may result in increased morbidity and mortality.8 Delay in antibiotic treatment of CAP, along with specific patient characteristics, can portend complications from continuing pneumonia despite appropriate antibiotic treatment, including parapneumonic effusions, empyema, and lung abscess, leading to unresolved acute pneumonia (URAP).
The symptoms and signs of CAP include a patient acutely feeling very ill or tired with accompanying fever and shaking chills, along with a cough producing purulent sputum; crackles, localized bronchial breathing, and decreased breath sounds; tachypnea (a respiration rate greater than 20 breaths/min); sinus tachycardia; and pleuritic chest pain.9
The key feature distinguishing acute pneumonia from chronic pneumonia is simply the sudden onset (hours to days) of symptoms in acute pneumonia and the late onset of symptoms in chronic pneumonia, with symptoms occurring for at least 6 weeks in the latter.
Mortality and severity prediction scores should be calculated and used to determine which patients should be hospitalized for CAP and which patients should be treated as outpatients.9
Patients with CAP are at risk for sepsis even after diagnosis and treatment with antibiotics. Fever, tachycardia, tachypnea, and altered consciousness are symptoms of sepsis that overlap with the clinical presentation of acute pneumonia; early diagnosis of CAP is therefore essential to avoid or forestall severe sepsis, septic shock, and death. Chest radiography is essential to confirm the diagnosis of acute pneumonia and to distinguish it from severe acute bronchitis. Computed tomography (CT) of the chest is generally not indicated unless a complication of CAP is suspected (eg, abscess, parapneumonic effusion, empyema).
MANAGEMENT
Early management of CAP is supportive with antipyretics and oxygen, if needed, and therapeutic with empiric antibiotics. Only the patient’s progress over the next 3 to 5 days can confirm whether the diagnosis and initial treatment are correct. It is a dangerous pitfall to think that antibiotic algorithms effectively cover the treatment of all pneumonias, because not all pneumonias are caused by bacteria or are even infectious (eg, extrinsic allergic alveolitis, pulmonary aspiration syndromes).10,11
Chest radiography and hospitalization of outpatients with CAP should be considered in patients who remain very ill after 48 hours of treatment with an antibiotic such as a macrolide or doxycycline.5 A respiratory fluoroquinolone, or cefpodoxime plus a macrolide, or amoxicillin-clavulanate plus a macrolide should be considered in outpatients with significant comorbidities (eg, chronic obstructive pulmonary disease [COPD], alcoholism) or who have used antibiotics in the previous 3 months.9
Empiric treatment of CAP in the hospital should include dual antibiotic therapy (eg, a β-lactam plus azithromycin or respiratory fluoroquinolone), particularly if the patient requires admittance to the intensive care unit.9 At the University of California, Davis, we recommend a third-generation cephalosporin (ceftriaxone), plus azithromycin or levofloxacin, with or without vancomycin (if methicillin-resistant Staphylococcus aureus infection is suspected), but the selection of empiric antibiotic treatment should always conform to the epidemiology of local infectious disease trends and antibiotic resistance patterns.
The majority of inpatients and outpatients with pneumonia feel better with the disappearance of fever and the lessening of productive cough within 3 to 5 days of initiation of antibiotics and supportive care. Other signs of resolving pneumonia include the disappearance of leukocytosis or leukopenia in 3 to 5 days and the patient’s restored ability to sleep well.
Radiographic resolution of acute bacteremic pneumococcal pneumonia should take no longer than 6 to 10 weeks and very often lags behind the patient’s clinical improvement.12 All patients with pneumonia should have follow-up chest radiography approximately 8 weeks after the initial diagnosis and treatment. If radiography findings have not returned to baseline after 8 weeks, consider the possibility of URAP. Follow-up chest radiographs are important, since CAP resolves radiographically by 4 weeks in only approximately 30% of patients older than 50 years.13,14
The current literature continues to cite the conventional wisdom that viral and “atypical” or uncommon pathogens such as Mycoplasma and Chlamydia tend to clear up on chest radiographs sooner than more common bacterial pneumonias.
Unless complications ensue in the hospital (eg, progressive pneumonia with development of effusions, empyema, acute respiratory failure, or septic shock), inpatients are discharged home after a median hospital length of stay of 5 days,8 with instructions to complete a full course of oral antibiotics. It is during this period of anticipated recovery from pneumonia that patients can develop URAP.
Important lessons can be learned from the time course of inpatients with CAP who fail to improve clinically during their hospital stay. Arancibia and colleagues found the following15:
- Antibiotic treatment failures were mainly infectious in origin, including primary, persistent, and nosocomial infections.
- Persistent infections were mostly due to microbial resistance to the administered empiric antibiotics.
- Nosocomial infections were very frequent among patients with progressive pneumonia and were the only cause of treatment failure to be independently associated with death.
Regardless of whether a patient with pneumonia is sent home from a clinic or emergency department or is hospitalized and later discharged home for acute pneumonia, 2 follow-up clinic visits are recommended. The first visit should take place approximately 1 week after initiating antibiotic treatment to ensure that symptoms of infection are disappearing and that normal activities of daily living are resuming. The second visit should take place approximately 8 weeks after initiating antibiotics and should include chest radiography to confirm radiographic resolution of pneumonia, or to confirm URAP.Increasingly shorter hospital stays in the United States may not work to pneumonia patients’ benefit. It is a very dangerous pitfall to treat and forget about patients with acute pneumonia once antibiotics have been initiated. Progressive pneumonia can kill a patient, so get patients back to the clinic for follow-up, and track them down if necessary.
NEXT: WHEN PNEUMONIA IS NOT IMPROVING
WHEN PNEUMONIA IS NOT IMPROVING
If pneumonia is not improving clinically or radiographically as would be expected at the second follow-up visit, the possibilities include recurrent pneumonia and URAP. Recurrent pneumonia is 2 or more separate episodes of new lower respiratory tract and lung tissue infection presenting with new fever, new leukocytosis, and new purulent phlegm. Recurrent pneumonia is typically separated by at least 1 month of clinical improvement or clearing of infiltrations on chest radiographs from the first acute CAP.16 URAP is the persistence of abnormal chest radiograph densities for more than 1 month in a patient with acute pneumonia who still has cough, dyspnea, fatigue, or fever.
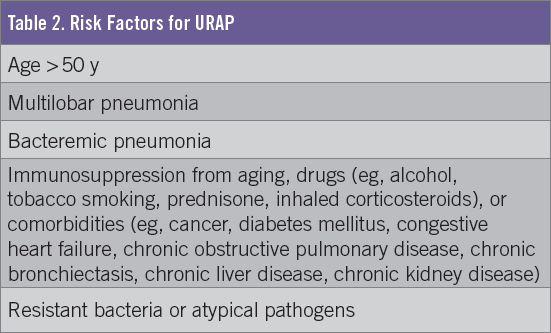
The most frequent reason for failure to respond to treatment in CAP is the progression of pathophysiologic changes despite appropriate antibiotic treatment.6 When a patient is failing to recover in the expected time period from the original acute pneumonia (Figure), consider the mnemonic “BAD OMEN” (Table 1) and recognize the risk factors for URAP (Table 2).


In the classic study by Jay and colleagues of patients with bacteremic pneumococcal pneumonia,12 lung consolidation had disappeared on chest radiographs in all 72 patients by 8 to 10 weeks, but in those patients with lung volume loss or pleural disease, radiographic resolution took more than 8 weeks. Interestingly, lung cancer was not a cause of delayed radiographic resolution. Age was found to be an independent risk factor for delay in radiographic resolution of pneumococcal pneumonia—90% of patients younger than 50 years resolved radiographically by 4 weeks, while only 30% of patients older than 50 years resolved by 4 weeks.12,13 Resolution on chest radiographs occurred earlier in the absence of comorbidities, specifically airway disease (such as COPD) and alcoholism, which slow radiographic resolution of CAP; lung cancer is a rare cause of delayed radiographic resolution of pneumococcal pneumonia.12
Bacterial pneumonia may take 1 to 6 months for chest radiograph findings to return to baseline. S pneumoniae, S aureus, and gram-negative bacteria such as L pneumophila can leave residual radiographic findings such as stranding in 10% to 35% of cases. Mycoplasma infection typically resolves in 2 to 4 weeks radiographically compared with bacterial pneumonias. If a patient is not improving as expected, think BAD OMEN, and order chest CT promptly.
The classic or most common presentation of noninfectious URAP—for example, bronchiolitis obliterans organizing pneumonia (BOOP) and hypersensitivity pneumonitis—is exactly the same as that of infectious pneumonia. The nonspecific signs, symptoms, and chest radiographic findings of bacterial, viral, or fungal pneumonias also occur in noninfectious pneumonia or pneumonitis. Fever, chills, night sweats, cough, difficulty breathing, fatigue, and infiltrates on chest radiographs occur with both etiologies. The presentation of noninfectious pneumonia or pneumonitis is so convincing for infection that most patients will have been treated with at least 1 course of antibiotics before an alternative (and correct) diagnosis is considered.
Procalcitonin is a helpful biomarker for infectious bacterial pneumonia; when the level is very low (< 0.1 ng/mL), bacterial infection is very unlikely, and this finding should prompt cessation of antibiotics and a search other reasons for URAP, such as viral pneumonia, pulmonary vasculitis, pulmonary embolism with pulmonary infarction, and even BOOP.17,18 Procalcitonin values between 0.10 and 0.25 ng/mL indicate that bacterial infection is unlikely, but clinical judgment is needed if the patient’s presentation is classic for acute pneumonia. A value greater than 0.25 to 2 ng/mL does not exclude bacterial infection, given that infection could be very localized such as with abscess. Repeating a procalcitonin test on days 3, 5, and 7 may be helpful in antibiotic stewardship, but this area remains murky.
MANAGEMENT OF URAP
URAP management includes high-resolution CT (HRCT) of the chest; consultation with a pulmonologist; bronchoscopy with bronchoalveolar lavage (BAL), with or without transbronchial lung biopsy and/or lymph node biopsy; and video-assisted thoracoscopic surgery (VATS) as a last resort. Microbiology and pathology test results are needed to determine the treatment plan.
The use of bronchoscopy with BAL, protected specimen brush catheters, and transbronchial lung biopsies can help diagnose the cause of URAP. In a small study of 35 patients at a single institution, bronchoscopy was diagnostic for a specific cause in 12 of 14 URAP cases.19 Bronchoscopy is the diagnostic procedure of choice for URAP, and chest CT scan is the roadmap for the bronchoscopist. Cancer, anaerobic bacteria, fungi, mycobacteria, and structural airway abnormalities are among the differential diagnoses listed in the BAD OMEN mnemonic. Larger lung biopsies such as with VATS may be necessary to confirm BOOP before initiating systemic corticosteroid treatment.20
Incomplete resolution or persistent radiographic infiltrates are concerning, and although consensus lacks on further management, we recommend proceeding with HRCT imaging of the lungs, which is well-established for diagnosing and managing many pulmonary diseases. The use of intravenous iodinated contrast is not recommended during HRCT, because subtle pulmonary findings may be obscured by intrapulmonary contrast. Prompt if not simultaneous consultation with a pulmonologist is also highly recommended to provide further insight and lessen the complications of URAP. Bronchoscopy and/or VATS may be required to differentiate the causes of URAP.
Laren Tan, MD, is an assistant professor of medicine at Loma Linda University School of Medicine in Loma Linda, California.
Samuel Louie, MD, is a professor of medicine in the Department of Internal Medicine, Division of Pulmonary, Critical Care, and Sleep Medicine, and director of the ROAD Center at UC Davis Medical Center in Sacramento, California.
REFERENCES:
- Reynolds AR. Pneumonia: the new “captain of the men of death.” Its increasing prevalence and the necessity of methods for its restriction. JAMA. 1903;XL(9):583-586.
- Armstrong GL, Conn LA, Pinner RW. Trends in infectious disease mortality in the United States during the 20th century. JAMA. 1999;281(1):61-66.
- Kochanek KD, Murphy SL, Xu J, Tejada-Vera B. Deaths: final data for 2014. Natl Vital Stat Rep. 2016;65(4):1-122.
- American Lung Association. Trends in Pneumonia and Influenza Morbidity and Mortality. http://www.lung.org/assets/documents/research/pi-trend-report.pdf. Published November 2015. Accessed July 21, 2017.
- Lim WS, Baudouin SV, George RC, et al. BTS guidelines for the management of community acquired pneumonia in adults: update 2009. Thorax. 2009;64(suppl 3):1-55.
- Barlett JG, Dowell SF, Mandell LA, File Jr TM, Musher DM, Fine MJ. Guidelines from the Infectious Diseases Society of America: practice guidelines for the management of community-acquired pneumonia in adults. Clin Infect Dis. 2000;31(2):347-382.
- Centers for Disease Control and Prevention. Achievements in public health, 1900-1999: control of infectious diseases. MMWR Morb Mortal Wkly Rep. 1999;48(29):621-629.
- Houck PM, Bratzler DE, Nsa W, Ma A, Bartlett JG. Timing of antibiotic administration and outcomes for Medicare patients hospitalized with community-acquired pneumonia. Arch Intern Med. 2004;164(6):637-644.
- Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44(suppl 2):S27-S72.
- Marik PE. Pulmonary aspiration syndromes. Curr Opin Pulm Med. 2011;17(3):148-154.
- Hu X, Lee JS, Pianosi PT, Ryu JH. Aspiration-related pulmonary syndromes. Chest. 2015;147(3):815-823.
- Jay SJ, Johnson WG Jr, Pierce AK. The radiographic resolution of Streptococcus pneumoniae pneumonia. N Engl J Med. 1975;293(16):798-801.
- Fein AM. Pneumonia in the elderly: overview of diagnostic and therapeutic approaches. Clin Infect Dis. 1999;28(4):726-729.
- Fein AM, Feinsilver SH, Niederman MS, Fiel S, Pai PB. “When the pneumonia doesn’t get better.” Clin Chest Med. 1987;8(3):529-541.
- Arancibia F, Ewig S, Martinez JA, et al. Antimicrobial treatment failures in patients with community-acquired pneumonia: causes and prognostic implications. Am J Respir Crit Care Med. 2000;162(1):154-160.
- Geppert EF. Chronic and recurrent pneumonia. Semin Respir Infect. 1992;7(4):282-288.
- Christ-Crain M, Müller B. Procalcitonin and pneumonia: is it a useful marker? Curr Infect Dis Rep. 2007;9(3):233-240.
- Delèvaux I, André M, Colombier M, et al. Can procalcitonin measurement help in differentiating between bacterial infection and other kinds of inflammatory processes? Ann Rheum Dis. 2003;62(4):337-340.
- Feinsilver SH, Fein AM, Niederman MS, Schultz DE, Faegenburg DH. Utility of fiberoptic bronchoscopy in nonresolving pneumonia. Chest. 1990;98(6):1322-1326.
- Epler GR. Bronchiolitis obliterans organizing pneumonia. Arch Intern Med. 2001;161(2):158-164.