
Recurring Violaceous Plaques on the Face of a 7-Year-Old
A 7-year-old African American girl presented to the emergency department with a history of recurrent episodes of hyperpigmented patches on the face during the past 6 months. With each new episode, the patches occurred on the same locations on the face. The patient’s mother explained that the patches would rapidly emerge within the course of several hours as dark, red-brown, dime- to quarter-sized lesions. Over the next few days, they would evolve into fluid-filled vesicles with a red-brown base, erode, and then resolve, leaving hyperpigmented patches.
The patient had tried applying beclomethasone dipropionate/clotrimazole cream, provided by a primary care physician, with minimal improvement in hyperpigmentation. By the time of presentation, the mother and primary care physician were alarmed by the recurrent nature of this unexplained rash. In fact, the patient had already been referred to a hematology-oncology specialist to evaluate for the possible presence of lymphomatoid papulosis.
The patient’s medical history was notable for seasonal allergies and well-controlled asthma, for which she was treated with a beclomethasone dipropionate inhaler as needed. Review of symptoms revealed no other significant findings.
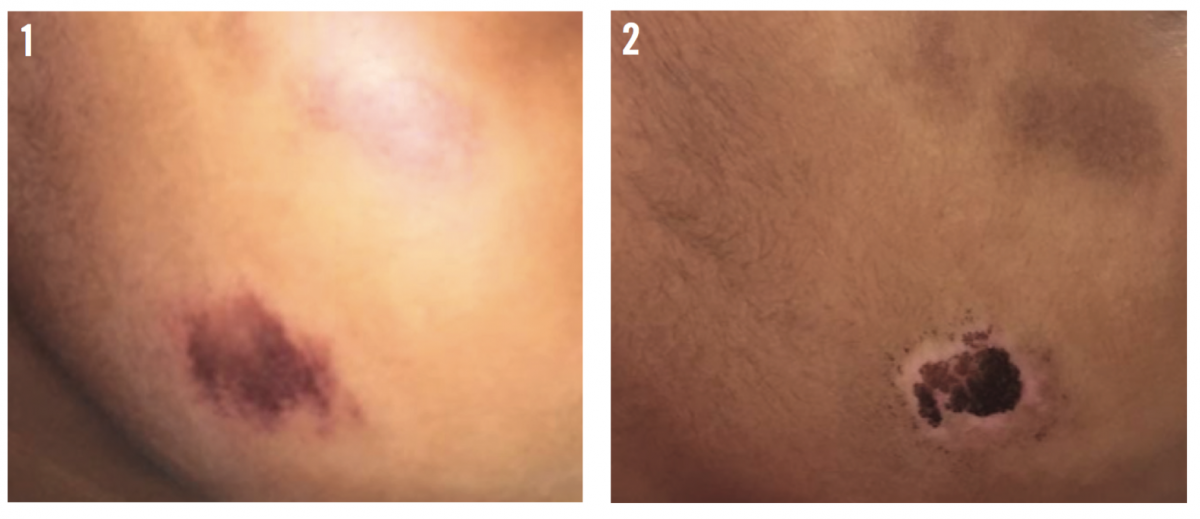
Upon physical examination, the patient was well-appearing and in no acute distress. On her lower right cheek, she had 1 quarter-sized, oval, violaceous to brown, thin plaque on an erythematous base, with minimal surrounding hypopigmentation. Several additional oval, brown, hyperpigmented patches with surrounding hypopigmentation also were seen on her cheeks, 1 on the superior right and 2 on the left (Figure 1).
Upon further questioning, it was revealed that 3 days before presentation, the patient had had a fever and had been treated with an over-the-counter children’s acetaminophen syrup. Further history revealed a likely temporal association between acetaminophen consumption and development of the rash.
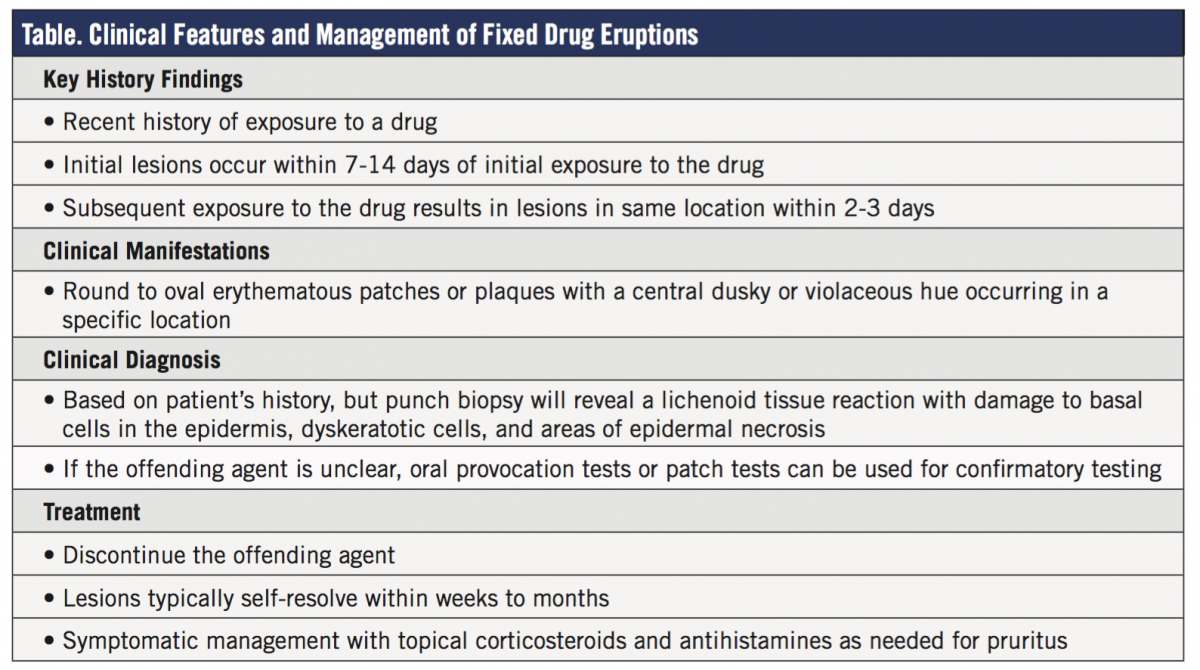
At a follow-up visit 5 days later, the initial patch on the girl’s right lower cheek had evolved to a superficial erosion with a central crust (Figure 2). An additional previously hyperpigmented patch on left lower cheek also had developed a superficial erosion.
(Answer and discussion on next page)
Answer: Fixed Drug Eruption
After careful consideration of the patient’s history and presentation, a clinical diagnosis of multiple fixed drug eruption (FDE) was made.
Results of a nasal swab test for Staphylococcus aureus were negative.
The patient was instructed to begin applying petrolatum to the affected areas on the face and to stop the beclomethasone/clotrimazole cream. She also was instructed to stop taking the acetaminophen syrup, and to keep a careful log of all medications, vitamins, and foods to which she was exposed.
Discussion
FDE is characterized by circular, hyperpigmented, violaceous plaques that occur in fixed areas in association with the exposure to a particular drug.1 With each new episode, the rash occurs in the same location; this is unique to FDE. In adults, it is the second most common cutaneous drug reaction after exanthematous rashes.2 In children, however, it is a rare or underdiagnosed condition.3
Upon exposure to an offending agent, lesions typically take 1 to 2 weeks to develop and can last for several days to weeks thereafter.1 Future exposure to the agent will produce the same reaction within 2 to 3 days.1 Although the pathophysiology of FDE is poorly understood, it is thought to involve the activation of intraepidermal CD8+ T cells that release immunologic mediators and respond more rapidly upon reexposure to the inciting antigen.4 In children, common culprits include sulfa-containing drugs, tetracycline, erythromycin, penicillin, metronidazole, loratadine, pseudoephedrine, barbiturates, potassium iodide, ibuprofen, and acetaminophen.5
Of note, synthetic coloring added to medications, especially tartrazine (FD&C Yellow No. 5), have been associated with FDE.6 Other medication dyes, including FD&C Blue Nos. 1, 2, and 7; Yellow Nos. 6 and 10; and Red No. 40 have been linked to adverse reactions.7 Our patient had ingested children’s acetaminophen syrup, which included Red No. 33 and Blue No. 1.
The clinical course of FDE is benign (Table), and lesions typically resolve within several weeks to months after discontinuing the offending agent.1 Patient education is key. Management includes emollients, topical corticosteroids, and oral antihistamines in cases involving pruritus.1
Jessica Mounessa, BS, is a fourth-year medical student and research fellow in the Department of Dermatology at the University of Colorado-Denver Anschutz Medical Campus in Aurora, Colorado.
Devorah Shagalov, MD, is a second-year resident in the Department of Dermatology at SUNY Downstate Medical Center in Brooklyn, New York.
Marjon Vatanchi, MD, is a pediatric dermatology research fellow in the Department of Dermatology at SUNY Downstate Medical Center in Brooklyn, New York.
Sharon Glick, MD, is the director of pediatric dermatology in the Department of Dermatology at SUNY Downstate Medical Center in Brooklyn, New York.
References
1. Flowers H, Brodell R, Brents M, Wyatt JP. Fixed drug eruptions: presentation, diagnosis, and management. South Med J. 2014;107(11):724-727.
2. Lee AY. Fixed drug eruptions: incidence, recognition, and avoidance. Am J Clin Dermatol. 2000;1(5):277-285.
3. Ponvert C, Rufin P, de Blic J. An unusual case of non-pigmenting fixed drug eruptions in a child. Pediatr Allergy Immunol. 2013;24(7):715-716.
4. Mahboob A, Haroon TS, Iqbal Z, Iqbal F, Saleemi MA, Munir A. Fixed drug eruption: topical provocation and subsequent phenomena. J Coll Physicians Surg Pak. 2006;16(12):747-750.
5. Dilek N, Özkol HU, Akbaş A, et al. Cutaneous drug reactions in children: a multicentric study. Postepy Dermatol Alergol. 2014;31(6):368-371.
6. Orchard DC, Varigos GA. Fixed drug eruption to tartrazine. Australas J Dermatol. 1997;38(4):212-214.
7. Swerlick RA, Campbell CF. Medication dyes as a source of drug allergy. J Drugs Dermatol. 2013;12(1):99-102.