
Photoclinic: Bedbug Bites

A 34-year-old woman presented with a blistering, intensely pruritic rash that had erupted 3 days earlier. Multiple papular lesions were densely clustered on areas of exposed skin (A). Excoriations were present, but there was no evidence of bacterial infection.
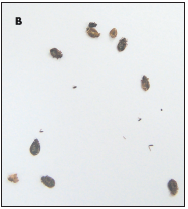
The patient had recently returned from a camping trip. At her campsite, she had noticed bugs crawling around her tent and had collected a few (B). Examination of the bugs led to a diagnosis of bedbug (Cimex lectularius ) bites.
Ronald Benjamin, MD, Jonathan Crane, DO, Patricia Hood, PA-C, Carla DiBenedetto, PA-C, and Kelly Mulligan, PA, of Wilmington, NC, remind us that the common bedbug is found in temperate regions worldwide. Although bedbugs are more frequently encountered in developing countries, infestations of US hotel rooms have been reported.
Similar in appearance to small cockroaches, bedbugs grow to about 5 mm and are reddish brown. These bloodsucking parasites feed mainly at night; they hide during the day in crevices, such as mattresses, box springs, and loose wallpaper. They feed for about 5 to 10 minutes per blood meal and can survive for long periods without eating. If a human host is not present, they will feed off any warm-blooded animal.1
 Bedbugs can serve as hosts for diseases such as hepatitis B, typhus, and anthrax. However, they are not able to transmit the causative organisms to humans; the principal problem with bedbugs is the inflammatory reaction from their bites. This reaction—which ranges from minimal erythema and pruritus to bullous lesions, severe pruritus, and purpura—most likely results from the saliva that is injected by the bedbug into the human during the bite.
Bedbugs can serve as hosts for diseases such as hepatitis B, typhus, and anthrax. However, they are not able to transmit the causative organisms to humans; the principal problem with bedbugs is the inflammatory reaction from their bites. This reaction—which ranges from minimal erythema and pruritus to bullous lesions, severe pruritus, and purpura—most likely results from the saliva that is injected by the bedbug into the human during the bite.
Bedbug bites generally require little treatment. This may include application of topical antiseptics, corticosteroid creams, and antipruritic lotions that contain menthol. Antihistamines are frequently used as well to reduce inflammation. In severe cases, oral corticosteroids are warranted. Insecticide should be used to eradicate a bedbug infestation.2
This patient was given oral prednisone, 40 mg every morning for 7 days, which was then tapered to 20 mg every morning for 7 days; in addition, she was told to apply triamcinolone acetonide (0.1%) cream twice daily for 2 weeks. After 1 week of treatment, the bullae had flattened, the pruritus had resolved, and only mild erythema remained. She finished her medications as prescribed.
REFERENCES:
1. Goddard J. Physician’s Guide to Arthropods of Medical Importance. 4th ed. New York: CRC Press; 2003:126-129.
2. Odom RB, James WD, Berger TG. Andrew’s Diseases of the Skin: Clinical Dermatology. 9th ed. Philadelphia: WB Saunders Co; 2000:552.