
Older Man With an Asymptomatic Lung Lesion
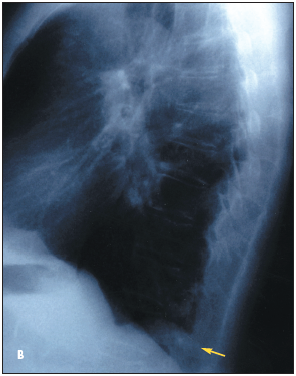
Routine chest radiographs reveal a left lower lobe density in a 70-year-old man (Figure 1 - Posteroanterior (A) and lateral (B) chest radiographs demonstrate a density in the left lower lobe). He has no chest pain, dyspnea, or hemoptysis.
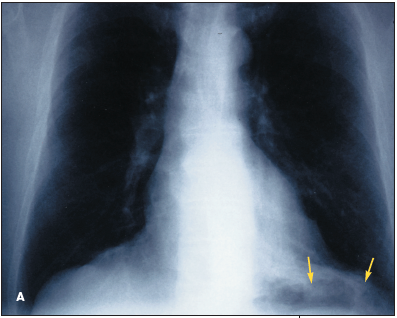
The patient has a 36-pack-year history of smoking. At age 22, he had a thoracotomy to repair damage to the left side of his diaphragm sustained in a fall from a bridge at age 7.
Vital signs are normal. Blood pressures in the upper extremities are equal. Pulses are equal and normal in all extremities. A bruit audible in the lower left posterior chest wall is loudest adjacent to the thoracotomy scar. There is no tenderness, palpable thrill, or pulsatile mass. Other cardiovascular findings are normal. He has no digital clubbing or cyanosis.
Arterial blood gases are normal (pH, 7.41; PaCO2 , 38 mm Hg; and PaO2 , 75 mm Hg). Hematocrit is 42%.
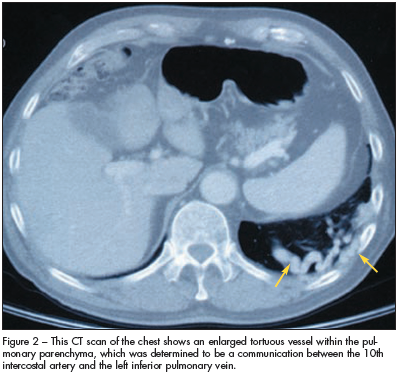
 A CT scan of the chest reveals an enlarged tortuous vessel within the pulmonary parenchyma (Figure 2). This vascular structure is interpreted as a communication between the 10th intercostal artery and the left inferior pulmonary vein. A pulmonary angiogram demonstrates no communication between a pulmonary artery and a pulmonary vein. A systemic to pulmonary arteriovenous fistula is diagnosed.
A CT scan of the chest reveals an enlarged tortuous vessel within the pulmonary parenchyma (Figure 2). This vascular structure is interpreted as a communication between the 10th intercostal artery and the left inferior pulmonary vein. A pulmonary angiogram demonstrates no communication between a pulmonary artery and a pulmonary vein. A systemic to pulmonary arteriovenous fistula is diagnosed.
Because the patient is asymptomatic, no treatment is required. He has had no complications from his arteriovenous fistula during 3 years of follow-up.
OVERVIEW: SYSTEMIC TO PULMONARY ARTERIOVENOUS FISTULA
Systemic to pulmonary arteriovenous fistulas are extremely rare.1 The first such case was reported in 1967.2
Although systemic to pulmonary arteriovenous fistulas of the thoracic cage can be congenital or can result from an inflammatory or neoplastic process, most are caused by missile penetration and stab wounds to the chest.1,3 Reported iatrogenic causes of thoracic systemic to pulmonary arteriovenous fistulas include chest-tube thoracostomy and resection of the lung.2,4
In this patient, it is not known whether the fistula was congenital or resulted from a traumatic injury sustained during his fall or his thoracic surgery.
The internal thoracic, internal mammary, and intercostal arteries, as well as anomalous branches from the aorta, have been reported to supply systemic to pulmonary arteriovenous fistulas. Drainage into the pulmonary arteries and veins occurs with equal frequency. Because most patients with this type of thoracic arteriovenous fistula are asymptomatic, this anomaly is usually detected incidentally during a routine physical examination or on imaging studies obtained for other reasons.3
DIAGNOSIS AND TREATMENT
 Since most systemic to pulmonary arteriovenous fistulas are caused by traumatic injury, they are generally recognized early and treated expeditiously.5 However, a systemic to pulmonary arteriovenous fistula may persist for years without consequence to the patient. Indications for intervention in chronic thoracic systemic to pulmonary arteriovenous fistulas have not been established.3
Since most systemic to pulmonary arteriovenous fistulas are caused by traumatic injury, they are generally recognized early and treated expeditiously.5 However, a systemic to pulmonary arteriovenous fistula may persist for years without consequence to the patient. Indications for intervention in chronic thoracic systemic to pulmonary arteriovenous fistulas have not been established.3
Nonetheless, it is important to determine which type of thoracic arteriovenous fistula is present. Because systemic embolization or hypoxemia may result from the shunting of blood through a pulmonary arterial to a pulmonary venous fistula, intervention should be considered in patients who have this type of thoracic vascular malformation. The results of this patient’s angiogram ruled out communication between a pulmonary artery and a pulmonary vein.
REFERENCES:
1. Coulter TD, Maurer JR, Miller MT, Mehta AC. Chest wall arteriovenous fistula: an unusual complication after chest tube placement. Ann Thorac Surg. 1999;67:849-850.
2. Cox PA, Keshishian JM, Blades BB. Traumatic arteriovenous fistula of the chest wall and lung. Secondary to insertion of an intercostal catheter. J Thorac Cardiovasc Surg. 1967;54:109-112.
3. Hirsch M, Maroko I, Gueron M, Goleman L. Systemic-pulmonary arteriovenous fistula of traumatic origin: a case report. Cardiovasc Intervent Radiol. 1983;6:160-163.
4. Fein AB, Godwin JD, Moore AV, et al. Systemic artery-to-pulmonary vascular shunt: a complication of closed-tube thoracostomy. AJR. 1983;140:917-919.
5. Yilmaz AT, Arslan M, Demirkilic U, et al. Missed arterial injuries in military patients. Am J Surg. 1997; 173:110-114.