
Managing Hypoandrogenism in the Aging Man
ABSTRACT: Hypoandrogenism is a common problem among aging men that is often underrecognized and underdiagnosed. Most men with the problem of low testosterone can be effectively treated with hormone replacement therapy, but further studies are warranted to document its safety in men with prostate cancer. This article will review the pathophysiology of hypoandrogenism, evaluating and diagnosing the condition, and the options for treating this common medical problem with testosterone replacement therapy.
Testosterone deficiency is a poorly understood condition that presents with few or nonspecific symptoms, and therefore remains underrecognized, especially in primary care settings where most men with symptoms are likely to be seen first. Testosterone deficiency, also known as hypogonadism or hypoandrogenism, increases with age. The exact prevalence of the syndrome is not known because of differences in clinical definitions across studies, but some studies estimate that approximately 20% of men in their 60s and 50% of men in their 80s with significantly low levels of serum total testosterone.1
However, greater recognition of the condition is paramount, as symptoms can be not only distressing and embarrassing for the patient, but also because low testosterone has been associated with increased cardiovascular risk. This article reviews the pathophysiology of hypogonadism, including late-onset hypogonadism. It also gives an overview of the different approaches to treatment with testosterone replacement therapy.
Defining Hypogonadism
Normal aging in men is associated with gradual and progressive decline of both serum total testosterone as well as bioavailable (nonsex hormone-binding globulin [non-SHBG]-bound) or free (non-SHBG non-albumin-bound) testosterone concentrations due to either primary testicular dysfunction or secondary hypothalamic-pituitary dysfunction.2-4 Primary androgen deficiency results from decreased production of testosterone by the Leydig cells within the testes and is characterized by decreased testosterone levels despite elevated gonadotropin-releasing hormone (GnRH) levels.5,6
Conversely, secondary androgen deficiency is the result of decreased GnRH secretion by the pituitary gland and is thus characterized by low levels of both testosterone and luteinizing hormone.4,5 Free or bioavailable testosterone displays an even more dramatic concentration decrease due to the concomitant increase in serum SHBG.3,5
Therefore, free or bioavailable testosterone levels, rather than total testosterone, may be a better indicator of true hypogonadism in older men since free testosterone levels decrease between 50% and 60% between the ages of 25 and 75 years, while total serum testosterone levels decrease only 35% in the same age span.6
• Causes of hypogonadism. Several chronic conditions, including renal failure, malignancy, diabetes mellitus, hyperthyroidism, hyperprolactinemia, HIV infection, and stress, can result in low testosterone levels.2,3,5,7,8 Many medications—primarily GnRH agonists and antagonists, estrogens, glucocorticoids, chemotherapy agents, thiazides, opiates, and many selective serotonin receptor inhibitors—can also decrease testosterone concentration.2,5 Orchitis and other testicular pathology or trauma can also lead to hypogonadism.3
Notably, there is an evident hereditary aspect to development of hypogonadism; genetics determines up to 60% of testosterone and 30% of SHBG concentration variability.3 Ultimately, the number of Leydig cells within the testes and the amount of testosterone each cell produces decreases with age and thus leads to low serum testosterone concentrations.9
Altered hypothalamic-pituitary function is also often observed, especially in obese individuals, which acts to compound the testicular deficiencies.9
• Late-onset hypogonadism. After age 30, an annual decrease in serum testosterone levels of approximately 1% occurs.5 As male life expectancy continues to increase, an increasing number of symptomatic men are considering androgen replacement therapy although well-validated criteria for diagnosis and treatment are lacking.6,10
Older men are likely to have proportionately greater incidence of primary hypogonadism, which has a direct link to aging while secondary hypogonadism occurs equally throughout age groups since it is correlated with obesity.6 Increased aromatization of testosterone to estradiol in adipose tissue, insulin resistance, and increased cytokine production in adipocytes are all linked to disrupting the hypothalamus-pituitary-gonadal axis in obese patients.6
Diagnosing Hypogonadism
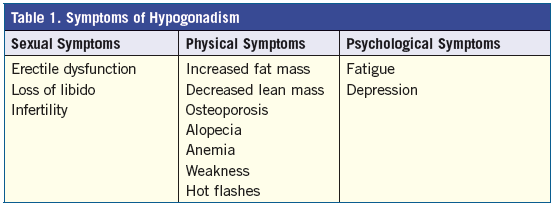
Patients with the condition may present with several different symptoms, which can be separated into 3 categories: sexual, physical, and psychological (Table 1).2,3,5,10In addition, laboratory testing can assist with making the diagnosis. Generally, serum testosterone levels between 300 ng/dL and 1000 ng/dL are considered within the normal range.2,11 The normal values for serum testosterone levels in men are outlined in Table 2.
More specifically, hypogonadism can be classified as testosterone levels below 320 ng/dL since normally healthy men between the ages of 20 and 40 years have serum concentrations above this level.3 Due to the negative side effects of supraphysiological levels of testosterone, sexual symptoms should be used in diagnosis only if low/normal serum levels are confirmed.2,3,10 Because 98% to 99% of testosterone is bound to either albumin or SHBG in the bloodstream, free or bioavailable testosterone is measured to provide a more accurate reading of the functional testosterone level.12
Luteinizing hormone and follicle-stimulating hormone concentrations should be recorded to distinguish between primary testicular hypogonadism and secondary hypothalamic-pituitary hypogonadism.5,12,13 Testosterone levels should be drawn in the morning, at their highest concentration due to circadian rhythms of secretion.5 Prolactin levels should also be measured in men with very low levels of testosterone (ie, <100 ng/dL) to rule out pituitary tumors.5,12,13

Treatment With Testosterone Replacement Therapy
Testosterone replacement therapy is most commonly used to treat hypogonadism, however, because of a lack of well-validated diagnostic criteria for testosterone deficiency, the type and dose of testosterone therapy is controversial.2,6,10 Testosterone supplementation is associated with an increase in lean body mass, decreased fat mass, increased bone density, improved mood and cognitive function, and enhanced libido and sexual function.2 Recent data suggests that declining levels of testosterone rather than high levels perhaps contribute to the genesis of benign prostatic hyperplasia and prostate cancer and that testosterone supplementation may actually decrease the incidence of these diseases.3,14
However, there are many contraindications to therapy, including a hematocrit level above 52%, untreated obstructive sleep apnea, severe lower urinary tract obstruction, untreated prostate cancer, benign prostatic hyperplasia, history of congestive heart failure, and men with a prostate-specific antigen (PSA) greater than 4.0 ng/mL.5 Serious side effects are not usually observed unless supraphysiological testosterone levels are reached.2-4 An increase in hematocrit and modest increases in PSA are the most common negative side effects, but most increases still remain within the normal ranges (PSA <4.0 ng/mL; hematocrit <50%).2,4
The most common ways to administer testosterone replacement therapy include long-acting intramuscular injections, transdermal gels and patches, and subcutaneous pellets—the pros and cons of which are reviewed in further detail below.5,15 Regardless of which route of administration is chosen, once testosterone treatment has started, regular clinical examination, including a digital rectal examination, hematocrit, and PSA, should be performed at least annually.9
• Injections. Injections are popular because they are safe, effective, and inexpensive; however, they may result in widely fluctuating levels of testosterone with supraphysiological peaks within 2 to 3 days of treatment and subphysiological troughs 12 to 14 days after injection.5,9,14,16 Intramuscular injections of long-acting testosterone enanthate or cypionate are administered every 2 to 3 weeks at doses of either 200 mg or 300 mg.14
Due to the widely varying concentrations, patients experience fluctuations in libido, sexual performance, and mood.14 Negative effects of intramuscular injections include pain associated with treatment, loss of circadian rhythm of testosterone levels, and suppression of luteinizing hormone secretion, which can lead to infertility.14
• Transdermal patches and gels. Transdermal testosterone preparations are more convenient for patients and cause fewer side effects by providing normal levels of androgens while maintaining circadian rhythms of testosterone concentration, but at a higher cost.3,5,9,14,17,18 Common side effects of transdermal treatment include skin irritation at the site of application because of allergic contact dermatitis, erythema, pruritis (especially with patches), and inadvertent transmission via skin contact of testosterone to women and children.9,14,17
Applying a small amount of 0.1% triamcinolone acetonide cream to skin can help reduce the incidence and severity of skin irritation without altering testosterone absorption.14 Additionally, most gel formulations include ethanol—which enhances absorption through the stratum corneum of the skin.18
Ethanol, which evaporates rapidly, is essential for efficient absorption of the hormone; therefore, after the alcohol has evaporated, absorption is greatly decreased.18 Consequently, individuals are advised to rinse the skin 10 minutes after application to minimize accidental transmission of the gel to women or children without altering the amount of bioavailable testosterone absorbed into the body.18
• Pellets. Testosterone pellets are arguably the most effective treatment for hypogonadism.15 The number of pellets are selected based on the serum testosterone level and they are implanted subcutaneously via either 100 mg or 200 mg pellets every 4 to 6 months into the buttocks.15 The implantation procedure takes between 10 and 15 minutes and is performed under local anesthetic.15 Once inserted, the pellets release between 1 mg to 2 mg per pellet of testosterone daily, which is sufficient to return serum concentrations to normal levels.19
Post-implantation follow-up is important to monitor testosterone and PSA levels.15 The main adverse effects of pellet implantation were bleeding at the injection site and infection, both of which are correlated with increased physical activity right after the procedure and greater number of pellets inserted.15
Use of Testosterone Therapy in Men With Prostate Cancer
The relationship of testosterone to prostate cancer has come under scrutiny recently due to an increase in prostate cancer survivors who present with symptoms of low testosterone.20 A direct correlation between testosterone levels and prostate cancer has never been shown; in fact the largest such study suggested that low testosterone levels may predispose men to an increased risk of prostate cancer.20,21
Prostate cancer rates in men undergoing testosterone replacement are approximately 1%, which is similar to the rates observed in the general population.20,21 Notably, prostate biopsies of hypogonadal men with normal digital rectal examination and PSA have a cancer rate of 14.3%, similar to the placebo rate of 15.2%.20,21
Low serum testosterone has been associated with more aggressive cancers and shorter survival rates after cancer treatment and the rate of cancer doubles in men with total testosterone levels less than 250 ng/dL.21 Particularly worrisome is the observation that men with low testosterone and PSA above 2 ng/mL are at particular risk for prostate cancer with a positive biopsy rate of 30.25%.21 This information demands additional research to determine whether low testosterone is a result or a cause of prostate cancer; if it causes cancer, research is needed to determine the level at which optimal testosterone saturation is reached to prevent cancer incidence.20,21
Hypoandrogenism is a common condition affecting millions of older men. The diagnosis can be made by observing clinical symptoms and by obtaining a serum testosterone level in the morning. Treatment with testosterone replacement therapy has shown to be effective, but consideration should be given to the appropriate route of administration with careful monitoring for adverse effects. The available evidence suggests that this treatment in men with prostate cancer does not pose an undue risk of prostate cancer recurrence or regression, but further controlled studies are needed to document its safety. ■
A Case Study
A 73-year-old man presented with loss of muscle mass, lethargy, and decreased libido for 5 years. He had adult onset diabetes mellitus, hypercholesterolemia, and symptoms of lower urinary tract symptoms. The physical examination revealed a moderately enlarged benign prostate gland, slightly atrophic testes, and a body mass index of 30. His serum testosterone level was 195 ng\dL. The cholesterol level was 250 mg\dL, and the glycated hemoglobin (HbA1C) was 6%. His hemoglobin level was 14.3 gm\dL. His PSA level was 2.7 ng\mL.
He was treated with intramuscular testosterone cypinoate 200 mg every 2 weeks. His serum testosterone level after 8 weeks of treatment increased to 450 ng\dL. His symptoms of lethargy and decreased libido improved but returned after 2 weeks of treatment. He was then offered daily application of testosterone gel, which markedly improved his symptoms without any rollercoaster effect that he experienced with testosterone injections.
PJ Kepper, BS, MS, is a graduate of Louisiana State University in Baton Rouge, LA, and has a Master’s degree in cellular biology from Tulane University in New Orleans, LA.
Neil Baum, MD, is a clinical associate professor of urology at Tulane Medical School in New Orleans, LA.
References:
1.Matsumoto AM. Fundamental aspects of hypogonadism in the aging male. Rev Urol. 2005;5(suppl 1):S3-S10.
2.Gruenewald DA, Matsumoto AM. Testosterone supplementation therapy for older men: Potential benefits and risks. J Am Geriatr Soc. 2003;51(1):101-115.
3.Oettel M, Hübler D, Patchev V. Selected aspects of endocrine pharmacology of the aging male. Exp Gerontol. 2003;38(1):189.
4.Calof OM, Singh AB, Lee ML, et al. Adverse events associated with testosterone replacement in middle-aged and older men: a meta-analysis of randomized, placebo-controlled trials. J Gerontol A Biol Sci Med Sci. 2005;60(11):1451-1457.
5.Baum NH, Crespi CA. Testosterone replacement in elderly men. Geriatrics. 2007;62(9):14-18.
6.
Tajar A, Forti G, O’Neill TW, et al; EMAS Group. Characteristics of secondary, primary, and compensated hypogonadism in aging men: Evidence from the European male ageing study. J Clin Endocrinol Metab. 2010;95(4):1810-1818.
7.Meaney AM, Smith S, Howes OD, O’Brien M, Murray RM, O’Keane V. Effects of long-term prolactin-raising antipsychotic medication on bone mineral density in patients with schizophrenia. Br J Psychiatry. 2004;184:503-508
8.Halbreich U, Kinon BJ, Gilmore JA, Kahn LS. Elevated prolactin levels in patients with schizophrenia: mechanisms and related adverse effects. Psychoneuroendocrinology. 2003;28(suppl 1):53-67.
9.Mudali S, Dobs AS. Effects of testosterone on body composition of the aging male. Mech Ageing Dev. 2004;125(4):297-304.
10.Wu FCW, 20 A, Beynon JM, et al; EMAS Group. Identification of late-onset hypogonadism in middle-aged and elderly men. N Engl J Med. 2010;363(2):123-135.
11.Carnegie C. Diagnosis of hypogonadism: Clinical assessments and laboratory tests. Rev Urol. 2004;6(suppl 6):S3-S8.
12.Dandona P, Rosenberg MT. A practical guide to male hypogonadism in the primary care setting. Int J Clin Pract. 2010;64(6):682-696.
13.Pantalone KM, Faiman C. Male hypogonadism: More than just low testosterone. Cleve Clin J Med. 2012;79(10):717-725.
14.Dobs SA, Meikle AW, Arver S, et al. Pharmacokinetics, efficacy, and safety of a permeation-enhanced testosterone transdermal system in comparison with bi-weekly injections of testosterone enanthate for the treatment of hypogonadal men. J Clin Endocrinol Metab. 199;84(10):3469-3478.
15.Handelsman DJ, Mackey MA, Howe C, Turner L, Conway AJ An analysis of testosterone implants for androgen replacement therapy. Clin Endocrinol. 1997;47(3):311-316.
16.Martin CW, Riley SC, Everington D, et al. Dose-finding study of oral desogestrel with testosterone pellets for suppression of the pituitary-testicular axis in normal men. Hum Reprod. 2000;15(7):1515-1524.
17.Nieschlag E. Testosterone treatment comes of age: new options for hypogonadal men. Clin Endocrinol (Oxf). 2006;65(3):275-281.
18.De Ronde W. Hyperandrogenism after transfer of topical testosterone gel: case report and review of published and unpublished. Hum Reprod. 2009;24(2):425-428.
19.Kelleher S, Howe C, Conway AJ, Handelsman DJ. Testosterone release rate and duration of action of testosterone pellet implants. Clin Endocrinol. 2004;60(4):420-428.
20.Morgentaler A. Testosterone and prostate cancer: an historical perspective on a modern myth. Eur Urol. 2006;50(5):935-939.
21.Mirone V. Testosterone and prostate cancer. European Genito-Urinary Disease. 2007:26-27.