
Low Back Pain: A Case of Malakoplakia
A 74-year-old man presented to his primary care provider with a 1-month history of new-onset low back pain. The patient was diagnosed with acute lumbago and was treated with muscle relaxants, nonsteroidal anti-inflammatory drugs (NSAIDs), and osteopathic manipulative treatment.
At his follow-up evaluation, the patient's symptoms did not improve and was also diagnosed with a urinary tract infection. He was treated with trimethoprim-sulfamethoxazole, and imaging studies were ordered.
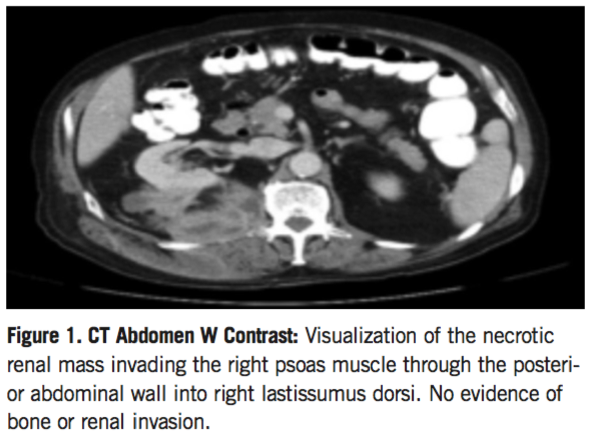
A computed tomography (CT) scan of the abdomen (Figure) and spine revealed a necrotic psoas mass arising from his right kidney, 10.1 × 3.5 × 8.0 cm. Upon further questioning, the patient admitted to a 30-lb weight loss over the course of several months. The patient was subsequently admitted to the hospital for concerns of an underlying neoplastic process.
His vital signs upon admission were stable, and physical examination revealed a 10-cm fluctuating right flank mass. His medical history was significant for myasthenia gravis, hypertension, hyperlipidemia, and chronic steroid use.
Laboratory Results. Pertinent laboratory findings included leukocytosis of 20,000 per mm3 and creatinine of 1.28 g/mol. Further, CT chest imaging showed a new 2-cm well-circumscribed right upper lobe lung nodule. The patient underwent a percutaneous drainage of the right renal abscess, a CT-guided lung biopsy, and a core renal biopsy.
The abscess culture grew Escherichia coli, and the patient was treated with intravenous piperacillin-tazobactam. The patient’s pulmonary nodule biopsy was nonmalignant and consistent with scar tissue formation.
The renal biopsy led to an initial diagnosis of oncocytoma, a benign renal neoplasm of perirenal tissue. However, the diagnosis of oncocytoma was inconsistent with the aggressive nature of the patient’s clinical condition, and the patient underwent a laparoscopic radical right nephrectomy. During the procedure, the right kidney and significant residual tissue was removed. The results of this concurrent renal biopsy revealed the final diagnosis of renal malakoplakia, a rare inflammatory condition. The patient improved and was discharged on levofloxacin for 16 days.
DISCUSSION >>
Discussion. Malakoplakia is a rare granulomatous inflammatory disease, characterized by intracytoplasmic Michaelis-Gutmann bodies on histology.2 The pathogenesis of Malakoplakia is unknown, but it is thought to result from the inadequate intracellular killing of phagocytosed bacteria by monocytes and macrophages.2 Histologically, this process is characterized by conglomerations of foamy histiocytes containing distinctive basophilic inclusions with surrounding clear halos known as Michaelis-Gutmann bodies.2 Malakoplakia frequently occurs in the genitourinary tract; however, cases of malakoplakia involving the colon, stomach, lung, and liver have been reported. The disease is also associated with E coli infection in 70% to 90% of cases,3 suggesting an impaired response to bacterial infection.
Underlying disease and immunosuppression is thought to play a role in malakoplakia, with approximately 21% of patients with malakoplakia having some form of defect in host defense.3The prevalence of the condition is unknown, but it is estimated that more than 700 cases have been reported in the literature.4
Our patient had a history of myasthenia gravis and was taking prednisone daily. Malakoplakia is often difficult to diagnose because of its rarity and varying histological picture.3 However, a definitive diagnosis depends on classic pathological findings.5 There is no established treatment for patients with malakoplakia, but research suggests that trimethoprim-sulfamethoxazole and fluoroquinolone are beneficial treatments because of their better penetration ability for intracellular bacteria.5 The treatment of choice, however, remains to be surgical intervention due to high cure rates (81%).2
Conclusion. To our knowledge and through an extensive literature review, malakoplakia is rare. It is often misdiagnosed due to the nature of the condition and its mimicry of other benign processes. This case highlights the importance of thoroughly investigating the cause of unresolving low back pain and the importance of visceral disease to be included in the differential diagnosis of low back pain. It is also imperative to ensure a patient's clinical presentation is consistent with the patient’s final diagnosis, especially when diagnosing rare pathologies.
References:
- Abolhasani M, Jafari AM, Asgari M, Salimi H. Renal malakoplakia presenting as a renal mass in a 55-year-old man: a case report. J Med Case Rep. 2012;6(379).
- Wielenberg AJ, Demos TC, Rangachari B, Turk T. case report malacoplakia presenting as a solitary renal mass. Am J Roentgenol. 2004:183(6)1703-1705.
- Kobayashi A, Utsunomiya Y, Kono M, et al. Malakoplakia of the kidney. Am J Kidney Dis. 2008;51(2):326-330.
- Daroux M. Malakoplakia summary. 2011. Available at: http://www.orpha.net/consor/cgi-bin/OC_Exp.php?lng=en&Expert=556. Accessed February 2015.
- Chen D, Hsu Y. Renal malacoplakia associated with diabetes mellitus. JTUA. 2004;15(2):70-73.