
Peer Reviewed
Idiopathic Hypogonadotropic Hypogonadism
Authors:
Zafar Qureshi, MD
UHI CommunityCare Clinic, Miami, Florida
Jacquelline Leva, DO
Westchester General Hospital, Miami, Florida
Syed A. A. Rizvi, PhD, MS, MBA, and Loan Le, BA, MS-IV
Nova Southeastern University, Fort Lauderdale, Florida
Muhammad A. Rehan, MBBS, MPH
Florida Department of Health, Fort Lauderdale, Florida
Syed A. Hassan
Florida International University, Miami, Florida
Citation:
Qureshi Z, Leva J, Rizvi SAA, Le L, Rehan MA, Hassan SA. Idiopathic hypogonadotropic hypogonadism. Consultant. 2018;58(5):e179.
A 40-year-old man presented with concern for erectile dysfunction (ED) and small genitalia size.
History. The man stated that he had had female phenotypic features since birth, including micropenis and cryptorchidism, the latter of which had been repaired hormonally. The patient denied genital pain, personality changes, or blurry vision. He also denied a history of the use of tobacco or any illicit substances. He reported that was unable to achieve an erection but could achieve ejaculation, although with a small volume.
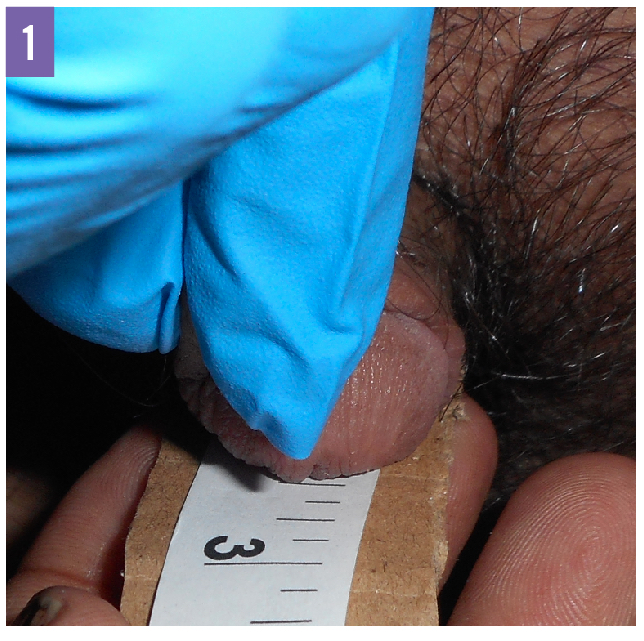
Physical examination. At presentation, the patient appeared anxious and in mild distress. His vital signs, including blood pressure, pulse, and respiratory rate, were normal, and he his heart rate and rhythm were regular. He had a height of 185.4 cm and weighed 102 kg, corresponding to a body mass index (BMI) of 29.7 kg/m2. He had a male body phenotype without gynecomastia. The flaccid penis measured 2.5 cm (Figure 1), and the testicles were relatively small in size. Neurological examination findings showed no cranial nerve conduction abnormalities and an intact sense of smell.
Diagnostic tests. Laboratory test results included a normal red blood cell count, white blood cell count, and hemoglobin A1c level. Levels of sodium, potassium, total calcium, albumin, aspartate transaminase, alanine aminotransferase, and creatinine also were within normal ranges.
Hormone test results included the following values: sex hormone–binding globulin, 28 nmol/L (reference range, 10-50 nmol/L); dihydrotestosterone, 14 ng/dL (reference range, 16-79 ng/dL); gonadotropin-releasing hormone (GnRH), less than 2.0 pg/mL (reference range, 0-10.0 pg/mL); testosterone, 31 ng/dL (reference range, 250-827 ng/dL); follicle-stimulating hormone, less than 0.7 mIU/mL (reference range, 1.6-18.0 mIU/mL); luteinizing hormone, less than 0.2 mIU/mL (reference range, 1.5-9.3 mIU/mL); and prolactin, 7.6 µg/L (reference range, 2.0-18.0 µg/mL).
Results of chromosomal studies showed a normal male karyotype (46,XY). Results of sperm studies of 2 specimens both revealed azoospermia. Results of magnetic resonance imaging (MRI) of the brain were normal, and abdominal and pelvic ultrasonography revealed normal anatomy.
Based on the patient’s history, physical examination findings, and laboratory test results, a diagnosis of idiopathic hypogonadotropic hypogonadism (IHH) was made.
Discussion. IHH is a genetic congenital disease that occurs predominantly in the male population, with a male to female ratio of 5 to 1. The condition results from a deficiency of GnRH and typically manifests as micropenis and hypogonadism, as well as cryptorchidism and ambiguous genitalia in many patients.1,2 Its estimated prevalence ranges from 1 in 10,000 to 1 in 86,000 men.3,4
IHH is divided into 2 categories based on the sense of smell. If the sense of smell is absent, it is referred to as anosmic hypogonadotropic hypogonadism or Kallmann syndrome; if the sense of smell is intact, it is called congenital normosmic IHH.4,5 Several genes, either alone or in combination, are implicated in GnRH deficiency, including ANOS1, FGFR1, PROK2/PROKR2, FGF8, GNRHR, CDH7, NSMF, KISS1/KISS1R, TAC3/TACR3, LEP/LEPR, and PCSK1.5-8
Patients who present with ED secondary to IHH can be treated with testosterone and human chorionic gonadotropin injections.8-10 We administered testosterone injections to our patient in order to decrease hormone therapy–related adverse events such as erythrocytosis, venous thromboembolism, acne, gynecomastia, and low sperm count. This treatment can partially correct micropenis without correction of sperm count.
With treatment, patients who are unable to have sexual intercourse secondary to anxiety over micropenis may have improved self-esteem and improved quality of life; for example, the increase in penis size greatly improved our patient’s reported quality of life. In addition, our clinic provided psychological and social counseling to help dissolve anxiety about his condition.
Treatment and outcome of the case. The patient began a regimen of testosterone injections. He received 2 mL of intramuscular (IM) testosterone for the first week, and then 1 mL IM once weekly for 6 weeks. After that period, his regimen was adjusted to a 2-mL testosterone injection biweekly. After 13 weeks of testosterone injection therapy, the patient’s penis measured 4 cm, a 1.5-cm increase from an initial length of 2.5 cm (Figure 2). Throughout this time, the patient’s libido was present and unchanged.

The testosterone injections were discontinued at the recommendation of a consulting urologist, and IM human chorionic gonadotropin was started at a dosage of 2 mL 3 times a week for 2 months in an attempt to further increase the size of the penis. The patient’s case will be followed to evaluate genitalia size increase and to monitor for adverse events related to long-term hormone therapy. Still, there is a question of whether the patient can maintain genital size with the cessation of weekly or biweekly testosterone treatment.
- Mao J-F, Nie M, Lu S-Y, Wu X-Y. Adult-onset idiopathic hypogonadotropic hypogonadism: possible aetiology, clinical manifestations and management. Asian J Androl. 2010;12(4):611-614.
- Seminara SB, Hayes FJ, Crowley WF Jr. Gonadotropin-releasing hormone deficiency in the human (idiopathic hypogonadotropic hypogonadism and Kallmann’s syndrome): pathophysiological and genetic considerations. Endocr Rev. 1998;19(5):521-539.
- Sumko D, Stoutt W, Weis SE, Wong L. Congenital idiopathic hypogonadotropic hypogonadism: a case report. J Clin Case Rep. 2014;4(6):371.
- Fraietta R, Zylberstejn DS, Esteves SC. Hypogonadotropic hypogonadism revisited. Clinics (Sao Paulo). 2013;68(suppl 1):81-88.
- Bianco SDC, Kaiser UB. The genetic and molecular basis of idiopathic hypogonadotropic hypogonadism. Nat Rev Endocrinol. 2009;5(10):569-576.
- Raivio T, Falardeau J, Dwyer A, et al. Reversal of idiopathic hypogonadotropic hypogonadism. N Engl J Med. 2007;357(9):863-873.
- Zhang Y, Zhang H, Qin Y, et al. Mutations in KISS1 are not responsible for idiopathic hypogonadotropic hypogonadism in Chinese patients. J Assist Reprod Genet. 2015;32(3):375-378.
- Hardelin J-P, Dodé C. The complex genetics of Kallmann syndrome: KAL1, FGFR1, FGF8, PROKR2, PROK2, et al. Sex Dev. 2008;2(4-5):181-193.
- Nerli RB, Guntaka AK, Patne PB, Hiremath MB. Penile growth in response to hormone treatment in children with micropenis. Indian J Urol. 2013;29(4):288-291.
- Kim S-O, Ryu KH, Hwang IS, Jung SI, Oh KJ, Park K. Penile growth in response to human chorionic gonadotropin (HCG) treatment in patients with idiopathic hypogonadotrophic hypogonadism. Chonnam Med J. 2011;47(1):39-42.