
ID Q&A: Treating Spider Bites: Is Dapsone an Option?
 Q: Some studies suggest that orally administered dapsone is effective for infections caused by spider bites (eg, brown recluse spiders) in dosages of 4 mg/kg/d for 3 days. Can dapsone be used in children and, if so, at what dosage?
Q: Some studies suggest that orally administered dapsone is effective for infections caused by spider bites (eg, brown recluse spiders) in dosages of 4 mg/kg/d for 3 days. Can dapsone be used in children and, if so, at what dosage?
--Ishkhan Babajanian, MD Santa Rosa, Calif
A: Treatments for brown recluse spider bites are controversial, and no conclusive test for envenomation is currently available. The majority of brown recluse spider bites heal without treatment within a few weeks or months.1,2 Patients with wounds that begin to show signs of tissue breakdown should receive prophylactic antibiotic therapy to prevent cellulitis.
 Bites that become necrotic and show signs of edema within hours of the bite may respond to dapsone-- a drug thought to be effective if administered early in the course of disease.1 The beginning dosage I use for children is 1 mg/kg given every 24 hours. This dosage may be increased if there is no response in 72 hours. Dapsone is approved for use in children. Side effects are dose-related hemolysis, sore throat, pallor, and very rarely, agranulocytosis. Some of these side effects are severe, and for this reason the drug should only be used in moderate to severe cases.3
Bites that become necrotic and show signs of edema within hours of the bite may respond to dapsone-- a drug thought to be effective if administered early in the course of disease.1 The beginning dosage I use for children is 1 mg/kg given every 24 hours. This dosage may be increased if there is no response in 72 hours. Dapsone is approved for use in children. Side effects are dose-related hemolysis, sore throat, pallor, and very rarely, agranulocytosis. Some of these side effects are severe, and for this reason the drug should only be used in moderate to severe cases.3
Corticosteroids have also been used to halt hemolysis with envenomation, to prevent kidney failure, and to reduce skin necrosis. When I treat patients, I use both dapsone and corticosteroids.
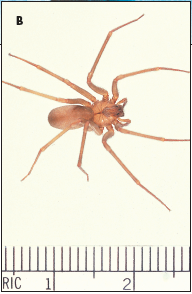
Figure – This child was bitten by a brown recluse spider 5 days before this photograph was taken (A). The characteristic marking of the true brown recluse spider is an upsidedown violin shape on the dorsal cephalothorax (B).
REFERENCES:
1. Stibich AS, Schwartz RA. Brown recluse spider bite. eMedicine. Available at: http://www.emedicine.com/derm/topic598.htm. Accessed July 27, 2005.
2. Anderson PC. Spider bites in the United States. Dermatol Clin. 1997;15:307- 311.
3. Wendell RP. Brown recluse spiders: a review to help guide physicians in nonendemic areas. South Med J. 2003;96:486-490.