
Peer Reviewed
A Photo Quiz to Hone Dermatologic Skills (Nov 2005)

Case 1:
A 60-year-old woman presents for evaluation of a patchy, slightly tender and pruritic rash on her trunk and proximal extremities. She has no history of a similar rash; however, she has had mild psoriasis on the elbows and knees. During a recent hospitalization for pneumonia, she received antibiotics as well as systemic corticosteroids. She recovered uneventfully; the psoriasis cleared during the hospitalization.
 What does this look like to you?
What does this look like to you?
A. Pustular drug reaction.
B. Staphylococcal folliculitis.
C. Pustular psoriasis.
D. Candida folliculitis.
E. Erythema multiforme.
Answer on next page
Case 1 Answer:
Pustular psoriasis, C, can be triggered by high-dose corticosteroid therapy in patients with longstanding stable plaque psoriasis. Treatment options for pustular psoriasis include topical calcipotriene, wet wraps, potent topical corticosteroids, acitretin, cyclosporine, and methotrexate.
Pustular psoriasis may be difficult to distinguish from a pustular drug reaction; a biopsy may be necessary to establish the diagnosis. Staphylococcal infections are usually more inflammatory and more tender. Candida folliculitis sometimes erupts after corticosteroid treatment; a culture or biopsy may be needed to distinguish it from pustular psoriasis. Erythema multiforme is not pustular.
Case 2 on next page
Case 2:
A 7-year-old boy has had an asymptomatic papular eruption on the trunk and extremities for several weeks. He is otherwise healthy.

What is your clinical impression?
A. Follicular eczema.
B. Pityrosporum folliculitis.
C. Lichen nitidus.
D. Lichen planus.
E. Keratosis pilaris.
Answer on next page
Case 2 Answer:
Lichen nitidus, C, a condition of unknown cause sometimes seen in children, generally lasts for several months before resolving. There is no known treatment.
Follicular eczema is usually seen only in atopic persons. Pityrosporum folliculitis is typically confined to the trunk. Lichen planus is pruritic and consists of flat purple polygonal papules. Keratosis pilaris preferentially affects atopic persons and is confined to the upper outer arms, upper outer thighs, and cheeks.
Case 3 on next page
Case 3:
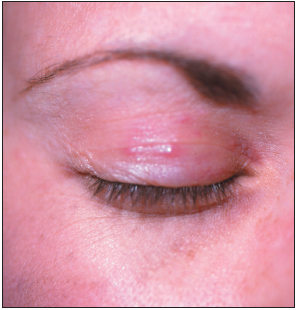 A 32-year-old woman has been bothered by an asymptomatic papular, erythematous eruption on her eyelids for several weeks. She has not changed her cosmetics or moisturizers. She denies rubbing her eyes or using eyedrops.
A 32-year-old woman has been bothered by an asymptomatic papular, erythematous eruption on her eyelids for several weeks. She has not changed her cosmetics or moisturizers. She denies rubbing her eyes or using eyedrops.
What is the most likely diagnosis?
A. Seborrheic dermatitis.
B. Rosacea.
C. Acne.
D. Sarcoidosis.
E. Syringomas.
Answer on next page
Case 3 Answer:
This patient has rosacea, B, which sometimes presents with eyelid lesions. The condition responded to a combination of topical antibiotics and oral tetracycline.
Seborrheic dermatitis may present with scaling, erythema, and blepharitis but not papules. Acne sometimes erupts on the eyelids, but an acneiform eruption as an isolated finding in a patient of this age would be highly unlikely. Papular lesions are frequently associated with sarcoidosis; however, other conditions would have to be ruled out before a diagnosis of sarcoidosis could be made. Syringomas—flesh-colored papules usually found on the lower eyelids—are benign eccrine gland tumors that begin to appear in the third and fourth decades. They are not erythematous.
Case 4 on next page
Case 4:
For 6 months, a 33-year-old woman has had a worsening acnelike condition. The outbreak initially cleared with mometasone cream, but the treatment is no longer effective. The patient has not started any new medications recently.
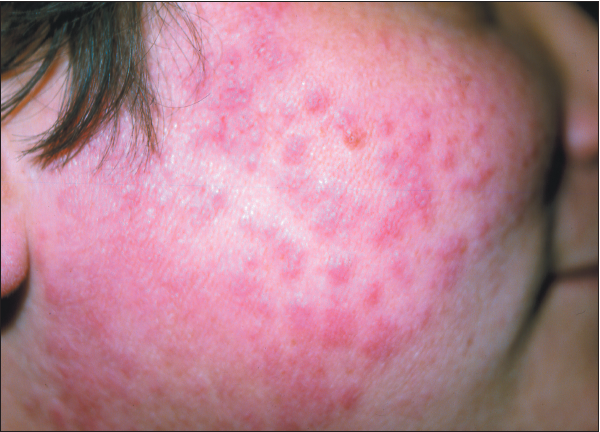
What do you suspect?
A. Rosacea.
B. Steroid rosacea.
C. Acne.
D. Cutaneous lupus erythematosus.
E. Keratosis pilaris.
Answer on next page
Case 4 Answer:
The patient has steroid rosacea, B. Initiation of treatment requires discontinuation of the topical corticosteroid; however, corticosteroid rebound may precipitate a flare of erythema and pustules that can persist for 6 to 8 weeks. Corticosteroid- sparing agents, such as tacrolimus or pimecrolimus, are recommended; antibiotics are sometimes used as well.
The patient’s history of corticosteroid use rules out acne and rosacea. Keratosis pilaris is usually seen in younger patients and typically is not highly inflammatory. Cutaneous lupus erythematosus might be considered; however, the patient has no history of photosensitivity.