
Commentary: Understanding the Importance of Time in Delivering Evidence-based Major Depression Treatment to Geriatric Patients in the Primary Care Setting
Introduction
By 2020, depression is expected to be the second most common cause of disability worldwide.1 Major depression will affect 4.9% to 17.9% of U.S. residents during their lifetime, and up to one-third of these persons will experience a chronic, relapsing course.2 The rate of depression in adults older than 65 years of age ranges from 7% to 36% in medical outpatient clinics.3 Depression in the elderly is widespread, often undiagnosed, and usually untreated.3 Fortunately, once a patient’s depression is diagnosed, effective treatments are available. Suffering can be reduced and depressive symptoms can be eliminated altogether in most persons by entering one of the several evidence-based forms of psychotherapy, by taking adequate doses of antidepressant medication, or by doing both.
In 2002, the U.S. Preventive Services Task Force (USPSTF) published its evidence-based recommendations for screening primary care patients for depression, stating that “Clinical practices that screen for depression should have systems in place to ensure that positive screening results are followed by accurate diagnosis, effective treatment, and careful follow-up. Benefits from screening are unlikely to be realized unless such systems are functioning well.”4 The effective application of the recommended diagnostic, treatment, and follow-up guidelines will undoubtedly take a considerable amount of the primary care provider’s and/or the collaborating mental healthcare provider’s time when the treatment of depression occurs in the primary care setting. This article discusses the time implications of using evidence-based treatment for depression on geriatric care practices.
Guidelines for Evaluation of Depression and Initiation of Pharmacotherapy
The Institute for Clinical Systems Improvement (ICSI) was established in 1993 by HealthPartners, the Mayo Clinic, and Park Nicollet Health Services. The ICSI brought leading medical experts together to rigorously develop evidence-based, best practice healthcare guidelines for the prevention, diagnosis, treatment, and management of numerous diseases and health conditions. According to the ICSI guideline, “Major Depression in Adults in Primary Care,” the initial evaluation of depression involves several important components, including3:
1. Suspect and screen for major depression
a. Use quantitative, standardized instruments to document depressive symptoms and track treatment response
b. Ensure that Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) criteria are present
2. Diagnose and characterize major depression with clinical interview
a. Screen for symptoms of major depression
b. Categorize severity of symptoms and degree of functional impairment
c. Obtain psychiatric history
1. Number and severity of previous depressive episodes
2. Response to previous treatment
3. Previous suicide attempts
d. Obtain history of psychosocial stressors
e. Rule out medical disorders that cause depression
f. Perform focused physical examination and laboratory testing as indicated
g. Determine medication history and history of substance abuse/dependence
3. Consider other mood and anxiety disorders or somatoform disorders
4. Assess patient for risk of harming himself or herself or others
5. Discuss treatment options and create treatment plan
6. Educate and engage patient with emphasis on the following topics:
a. Cause, symptoms, and natural history of major depression
b. Treatment options (eg, pharmacotherapy, psychotherapy, exercise)
c. What to expect during course of treatment (eg, duration, number of sessions, dosage, side effects, timing of symptom response)
d. How to monitor symptoms and side effects of treatment
e. Follow-up protocol (eg, office visits, telephone contacts)
f. Early warning signs of relapse or recurrence
g. Length of treatment
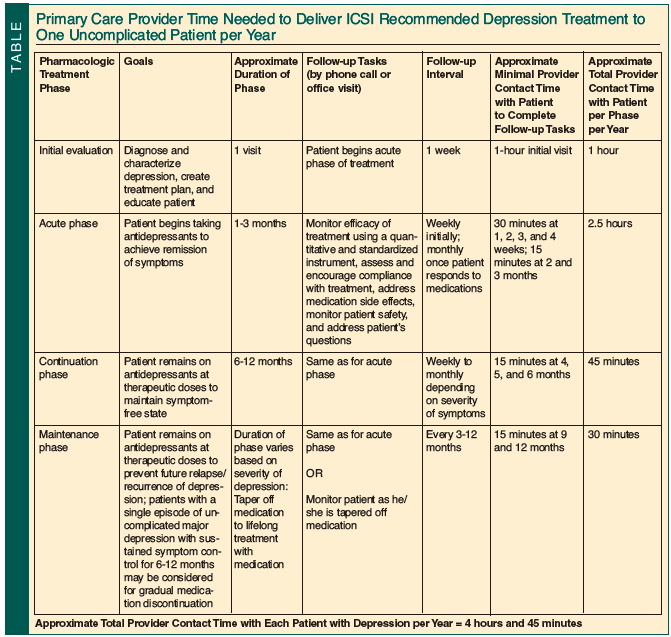
While the duration of such an initial assessment will vary, a thorough evaluation incorporating the ICSI recommendations would take, on average, 1 hour to complete (Table). Included in that time is the initiation of a therapeutic relationship with the patient and the development of rapport.
Guidelines for Pharmacotherapy: Acute Phase of Treatment of Depression
During the acute phase of pharmacotherapy, patients begin taking antidepressant medications in order to achieve remission of major depressive symptoms. It takes approximately 1 to 3 months for the remission of symptoms to occur, but in elderly populations, it may take even longer.3 Patients will often require titration of dosages of their antidepressant medications to achieve remission. The ICSI recommends that follow-up with patients with depression should initially occur weekly; contacts can then extend as far as monthly once the patient is responding to medications.3 Follow-up contact should address the side effects of medications, determine if the patient is following through on his or her treatment plan, and monitor the efficacy of treatment.3 To accomplish the patient education and monitoring recommendations of the ICSI during the acute therapy period, primary care providers would need at least 2.5 hours of contact time per patient with depression annually (Table).
Guidelines for Pharmacotherapy: Continuation Phase of Treatment for Depression
During the continuation phase of treatment, patients remain on therapeutic doses of antidepressant medication for the amount of time required to maintain a symptom-free state. According to the ICSI, this phase lasts at least 6 months, but preferably will last up to 1 year.3 Patients continue to require follow-up (by phone or in person) to address the side effects of medications, to determine if they are following through on their treatment plan, and to monitor the efficacy of treatment.3 The ICSI recommends that follow-up of patients with depression should occur weekly to monthly during this phase, depending on the severity of symptoms.3 To accomplish the patient education and monitoring recommendations of the ICSI during the continuation therapy period, primary care providers would need at least 45 minutes of contact time per patient with depression annually (Table).
Guidelines for Pharmacotherapy: Maintenance Phase of Treatment of Depression
During the maintenance phase of treatment, the dose of antidepressant medication that leads to satisfactory acute therapeutic response is maintained long-term to prevent relapse and the recurrence of depression. The duration of this phase depends on the severity and number of episodes of depression. The ICSI recommends that patients with a single episode of major depression with sustained symptom control for 6 to 12 months be considered for gradual medication tapering and discontinuation.3 More than 1 episode of depression requires longer periods of maintenance therapy, depending on the number of episodes.3 Once maximal symptom improvement has occurred, the ICSI recommends that the primary care provider see the patient, on average, every 3 to 12 months while he or she is on medication to monitor for symptom recurrence.3 Patients who do not require maintenance medication still need to follow up with their primary care provider as they are tapered off of medication. If primary care providers only spend an average of 15 minutes per visit while tapering patients off of antidepressant medication, it would require an additional minimum of 30 minutes of provider time annually (Table). Of course, those with chronic and/or intermittent major depression may require increased visit duration and/or frequency.
Evidence-based Psychotherapy Modalities for Treatment of Depression
There are specific time-limited psychotherapy modalities, including cognitive behavioral therapy and interpersonal psychotherapy, among other therapies, that have been shown to be effective for the treatment of depression.5 Patients who choose these psychotherapy options, either alone or with pharmacotherapy, require 12 to 20 weekly, hour-long therapy sessions for the treatment of depression to be effective.5 Although psychotherapy is initially time-intensive, time-limited psychotherapies may not need to be continued to maintain their effect, unlike medications. While primary care providers typically do not have the proper training to provide such interventions, they do have an obligation to assist patients in finding a therapist who is appropriately trained in the use of these specific forms of psychotherapy. Further, there should be continuous collaboration between the psychotherapist and the primary care provider to optimize patient therapeutic outcomes.
Effect of Evidence-based Care for Major Depression Treatment on General Medical Physician Practice and Clinic Organization
If primary care providers averaged 50 hours of work per week, assuming they took 3 weeks of vacation per year and had no administrative activity, they would have approximately 2450 hours of patient contact time per year. The panel size for a full-time family physician taking care of his or her own patients in a mature system can be up to approximately 2500 patients.6 If each provider carried 2500 patients in his or her panel, approximately 225 patients would have major depression, based on a 9% prevalence rate.7 It would take 1069 hours of primary care provider time per year to treat the 225 patients with depression (225 patients with major depression multiplied by 4.75 provider hours per patient with depression per year [Table]). If primary care physicians chose to use evidence-based pharmacotherapy to treat their patients with depression themselves rather than referring them to a specialist, up to 44% of the clinicians’ time (1069 hours divided by 2450 total patient contact hours) would be reallocated to depression treatment.
Although psychotherapy is equally effective as pharmacotherapy in the management of mild-to-moderate depression, psychotherapy takes up more of the practitioner’s time. Again, assuming 2450 total patient contact hours per year, one psychotherapist would be able to treat a maximum of 204 patients with depression per year (2450 total patient contact hours divided by the minimum of 12 therapist hours needed per patient with depression per year). If psychotherapists treated their patients with 20 weekly hour-long sessions, they would only be able to treat 122 patients with depression per year. Between 1.1 and 1.8 therapists would be required for each primary care provider to only treat the mental health needs of patients with depression (225 patients with depression per primary care panel divided by 122 to 204 patients treated per therapist).
This article takes a very conservative look at the time it takes to provide evidence-based antidepressant pharmacotherapy and/or psychotherapy for patients with uncomplicated and intervention-responsive major depression. There is obviously a wide variation in the number and types of psychotherapy that could be used, medications that could be given, and responses that could be expected. During all phases of treatment of depression, it is necessary for the primary care provider to spend time with the patient to maintain adherence to medical care recommendations and to provide support and crisis intervention during this time of emotional instability. While mood stabilization is the primary goal, patients often also need help in re-establishing normal family interactions, returning to work, and regaining other functions of normal living; thus, the time estimates in the Table are likely underestimated. This crude approach, however, provides an interesting and informative glimpse into the impact that depression treatment in the primary care setting would have if the goal was to actually improve both medical and mental health outcomes rather than to merely expose patients to the current system of “hit or miss” mental health interventions.8
Collaborative Care Model for Treatment of Depression
Adults should see a primary care physician an average of 40 minutes per year to receive adequate preventive care.9 In addition, there is an anticipated average need of 20 to 40 minutes annually for each chronic condition a patient may have.10 Since more than half of U.S. primary care physicians’ time is spent on the management of acute conditions,11 providers would already be at 1.5 times the contact hours available for care before even considering the addition of evidence-based depression treatment. Simple addition and multiplication suggests that it would not be possible to add this responsibility without decreasing panel size or altering the type of assistance that is available to treating practitioners as they provide evidence-based care to their patients.
One proven way that primary care providers can implement the guidelines recommended by the ICSI without dramatically affecting an already oversubscribed primary care provider’s work schedule is through the use of a collaborative care model for the treatment of depression. Such a redesign in the organization of a general medical clinic would include a team-based collaborative care approach in which a care manager, a primary care physician, and a consulting psychiatrist would work together to provide depression education, self-management support, active intervention with referral for psychotherapy when needed, and treatment response monitoring. The effectiveness of the collaborative care model for improvement in treatment adherence, patient quality of life, and depression outcomes has been demonstrated in more than 37 randomized, controlled trials.3 Further, the Improving Mood: Promoting Access to Collaborative Treatment (IMPACT) program for late-life depression was found to be associated with reduced total healthcare service use and cost reduction as compared with usual primary care during the 4-year study period.12
In the collaborative care model, care managers coordinate and assist in the treatment of patients with depression and other chronic illnesses. They maintain contact with the patient; provide educational material, self-management tools, and tips; answer questions; assure intervention adherence; and follow patient improvement. When complications arise or treatment is not helping, care managers consult with a psychiatrist or other specialist as a collaborative effort with the primary care provider. The care manager is a trained member of the primary care provider’s interdisciplinary team. One of the challenges that face primary care providers who are trying to single-handedly provide effective evidence-based care to patients with major depression is finding time to incorporate proven management strategies. The use of a collaborative care model and the transition of much of the responsibilities involved with patient education, follow-up, and care coordination to a care manager ensure that evidence-based recommendations such as those from the ICSI are implemented in a fashion that saves the primary care provider’s time while improving the patient’s health and curbing total healthcare costs.
Conclusion
While depression is well appreciated as a health issue, in general medical patients—and particularly those with chronic illnesses—major depressive illness remains underdiagnosed,13 treatment is largely limited to the use of medication with little in the way of follow-up care,8 and access to mental healthcare referral sources is limited.8 The use of a collaborative care model in the treatment of patients with depression ensures that evidence-based recommendations are carried out correctly and efficiently.
The authors report no relevant financial relationships.
Dr. Talebreza Brandon is Clinical Instructor of Geriatric Medicine, University of Utah, Salt Lake City, and Physician Investigator, the Department of Veterans Affairs Medical Center, Salt Lake City, UT; Dr. Bair is Professor of Geriatric Internal Medicine and Geriatric Psychiatry, University of Utah, Salt Lake City, and is Physician Investigator, the Department of Veterans Affairs Medical Center, Salt Lake City, UT; and Dr. Kathol is Adjuvant Professor of Internal Medicine and Psychiatry, University of Minnesota, Minneapolis.
References
1. Geddes J, Butler R, Hatcher S, et al. Depressive disorders. Clin Evid 2004;(12):1391-1436.
2. Rush AJ, Trivedi M, Fava M. Depression, IV: STAR*D treatment trial for depression. Am J Psychiatry 2003;160(2):237.
3. Institute for Clinical Systems Improvement. Health care guideline: Major depression in adults in primary care. Thirteenth Edition. May 2010. http://www.icsi.org/depression_5/depression__major__in_adults_in_primary_care_3.html. Accessed December 15, 2010.
4. U. S. Preventive Services Task Force. Screening for depression. Recommendations and rationale. U. S. Preventive Services Task Force (USPSTF). http://www.uspreventiveservicestaskforce.org/3rduspstf/depression/depressrr.pdf. May 2002. Accessed December 15, 2010.
5. Markowitz JC. Evidence-based psychotherapies for depression. J Occup Environ Med 2008;50(4):437-441.
6. Murray M, Tantau C. Same-day appointments: Exploding the access paradigm. Fam Pract Manag 2000;7(8):45-50.
7. Katon W, Schulberg H. Epidemiology of depression in primary care. Gen Hosp Psychiatry 1992;14(4):237-247.
8. Callahan CM. Depression in primary care: Encouragement and caution for the business case. J Gen Intern Med 2006;21(10):1125-1127.
9. Yarnall KS, Pollak KI, Østbye T, Krause KM, Michener JL. Primary care: Is there enough time for prevention? Am J Public Health 2003;93(4):635-641.
10. Østbye T, Yarnall KS, Krause KM, Pollak KI, Gradison M, Michener JL. Is there time for management of patients with chronic diseases in primary care? Ann Fam Med 2005;3(3):209-214.
11. Stange KC, Zyzanski SJ, Jaén CR, et al. Illuminating the ‘black box.’ A description of 4454 patient visits to 138 family physicians. J Fam Pract 1998;46(5):377-389.
12. Unützer J, Katon WJ, Fan MY, et al. Long-term cost effects of collaborative care for late-life depression. Am J Manag Care 2008;14(2):95-100.
13. Simon GE. Treating depression in patients with chronic disease: Recognition and treatment are crucial; depression worsens the course of a chronic illness. West J Med 2001;175(5):292-293.