
Chronic Obstructive Pulmonary Disease: Is It a Systemic Disorder?
ABSTRACT: Chronic obstructive pulmonary disease (COPD) typically is considered a disease of the lungs, but in actuality, it is a complex, multicomponent disease that can affect different systems. An abnormal inflammatory response of the lungs to noxious substances, such as cigarette smoke, is the primary factor contributing to development of airflow limitation characteristic of the disease. However, COPD also is associated with systemic inflammation, which may be linked to the observed significant extrapulmonary effects, including muscle wasting and cachexia, cardiovascular disease, osteoporosis, depression and anxiety, and anemia, which contribute to poor outcomes in some patients. These comorbidities have to be considered and managed in conjunction with COPD treatment for a more holistic approach in order to improve patients’ overall health. Because systemic inflammation may be an important contributor to the comorbidities associated with the disease, future systemic anti-inflammatory therapies may play a role in targeting the extrapulmonary effects of COPD.
_______________________________________________________________________________________________________________________________
Airflow limitation that is characteristic of chronic obstructive pulmonary disease (COPD) results from a variety of contributing factors in the lungs, including mucociliary dysfunction, pulmonary structural changes, and airway inflammation.1 Airway inflammation in patients with COPD most commonly originates from chronic exposure to noxious stimuli, including cigarette smoke, air pollution, and burning of wood or biomass fuels.2 It involves activated neutrophils, macrophages, and CD81 T-cell lymphocytes, and increased levels of inflammatory mediators, including leukotriene B4, interleukin (IL)-8, and tumor necrosis factor-a (TNF-a).2 COPD is also associated with clinically relevant extrapulmonary effects, including poor nutritional status, muscle wasting, and impaired skeletal muscle function,3 which may further contribute to disease severity in some patients.2 Several other comorbidities also can contribute to disease severity and/or complicate COPD management.2 Systemic inflammation has been pro-posed as a pathogenic link between COPD and some of these comorbidities, such as osteoporosis and cardiovascular disease.4-7
EVIDENCE AND ORIGINS OF SYSTEMIC INFLAMMATION
Although it is well known that COPD is associated with chronic airway and lung inflammation,2 increased levels of oxidative stress,8,9 activated inflammatory cells,10-12 and proinflammatory cytokines13 are also seen in the systemic circulation of COPD patients compared with healthy individuals.3 Serum levels of C-reactive protein (CRP), a marker of inflammation that has been shown to predict cardiovascular events,14 and of TNF-a, a marker of muscle wasting in patients with cancer,15 are elevated in COPD patients compared with smokers without COPD,16,17 and these levels appear to rise with increasing COPD severity.18 Increased CRP levels have also been shown to be associated with COPD-related hospitalization and death.19
Several origins of the systemic inflammation in COPD have been proposed. In the “spillover hypothesis” (Figure), inflammation begins in the lungs following the exposure to tobacco smoke or other oxidants, worsens with increasing airflow obstruction,20 and spreads to the systemic circulation via inflammatory cells and mediators, potentially causing the extrapulmonary manifestations.20 Although chronic exposure to cigarette smoke is the most common risk factor for COPD,2 genetic predisposition and gene-environment interactions also may contribute to COPD susceptibility.2 According to the “susceptible host hypothesis,” injury from tobacco smoke or other oxidants propagates inflammation in multiple organs including the lung, leading to small airway narrowing and other COPD manifestations in susceptible individuals.21 Other potential origins for systemic inflammation include lung hyperinflation, tissue hypoxia, and sympathetic and neurohormonal activation.20

SYSTEMIC COMORBIDITIES OF COPD
Systemic comorbidities are common in patients with COPD and can lead to an increase in the level of disability associated with the dis-ease.2 Categories of comorbidities include those with common pathways, including other smoking-related diseases such as ischemic heart disease and lung cancer, and those considered to be complications of COPD, including pulmonary hypertension and heart failure.2 Coexisting coincidental comorbidities, such as bowel or prostate cancer, depression, diabetes, dementia, Parkinson’s disease, and arthritis, are pathogenically unrelated, but they can complicate COPD management.2 Intercurrent comorbidities, including upper respiratory tract infections, are acute illnesses that may have a more se-vere impact in COPD patients com-pared with those without COPD.2
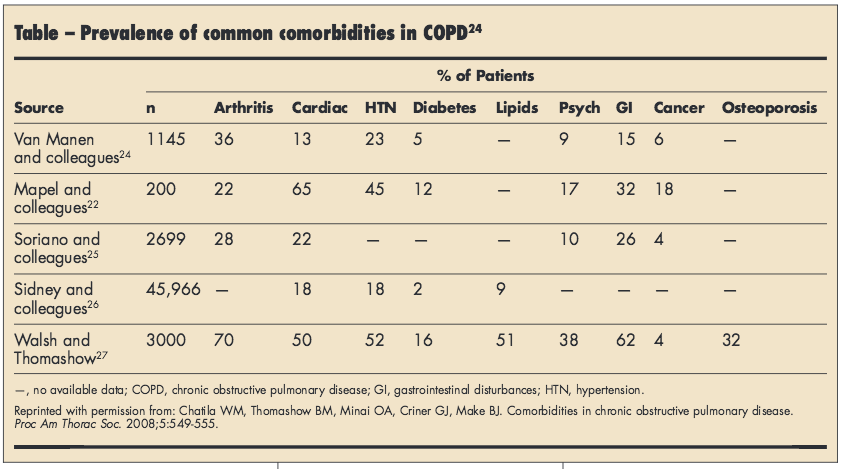
In a large study of 2 population-based National Institutes of Health cohorts, patients with severe or very severe COPD were more likely to have 1, 2, or 3 comorbid conditions compared with participants with normal lung function.22 In a case-control study, only 6% of 200 patients with COPD did not have another chronic medical condition. Patients with COPD and healthy controls had an average of 3.7 and 1.8 chronic medical conditions, respectively (P < .001).23 Frequent comorbidities of patients with COPD include arthritis, cardiac disorders, hypertension, diabetes mellitus, lipid disorders, psychiatric conditions, gastrointestinal diseases, cancer, and osteoporosis (Table).24-28
Muscle wasting and cachexia. The prevalence of nutritional deple-tion and associated weight loss has been shown to increase with increas-ing severity of COPD,29 and low and normal weight is associated with decreased survival compared with overweight and obese patients with COPD.30 Loss of muscle mass is a primary reason for weight loss in patients with COPD.3 A study of muscle biopsies from 15 patients with COPD and 8 healthy participants showed an increased percentage of apoptotic cells in patients with COPD versus healthy controls and in COPD patients with low versus normal body mass index (BMI).31
Skeletal muscle dysfunction has many potential causes, including physical inactivity, nutritional deple-tion, tissue hypoxia, oxidative stress, and systemic inflammation.3 In-creased levels of circulating CRP, IL-6, TNF-a, and other inflammatory mediators have been detected in COPD patients with skeletal muscle wasting versus normal skeletal muscle mass.32 Increased circulation of TNF-a leads to apoptosis and loss of protein in skeletal muscle cells.33,34 Patients with COPD often have an increased basal metabolic rate3,34 and commonly experience cachexia, which is a “wasting syndrome” involv-ing weight loss, skeletal muscle atrophy, and weakness that is associated with systemic inflammation.33 Cachexia is an important predictor of mortality and is associated with functional impairment and reduced quality of life.34 These findings highlight the importance of implement-ing and maintaining pulmonary rehabilitation programs, including exercise training and nutrition counseling, in appropriate patients early in the disease process.2
Cardiovascular disease. The lung and the heart are physiologically integrated and functionally interdependent.35 The increased work of breathing associated with COPD is particularly problematic in patients with compromised cardiac function because greater cardiac output is required.35 In addition, the pres-ence of COPD can impair cardiac function because pulmonary hypertension leads to increased cardiac strain.35 Evidence suggests a connection between cardiovascular complications and systemic inflammation associated with COPD.36 Circulating levels of TNF-a or CRP as a result of chronic lung inflammation may accelerate development of atherosclerosis.35 High levels of circulating CRP and severity of airflow obstruction have also been correlated with in-creased risk of cardiac infarction in patients with COPD.5
Patients with COPD are indeed at increased risk for cardiovascular complications and cardiovascular dis-ease.37,38 Compared with healthy controls, patients with COPD have increased arterial stiffness,38 which is an independent predictor of cardiovascular complications.39 In addition, COPD patients have a significantly higher prevalence of and greater risk of hospitalization for arrhythmia, angina, acute myocardial infarction, congestive heart fail-ure, stroke, and pulmonary embolism compared with controls.37 In the Towards a Revolution in COPD Health (TORCH) trial,40 27% of all deaths were due to cardiovascular disease,41 which is consistent with findings from other studies in patients with COPD (see Chatila and colleagues24 for a summary of studies). Moreover, patients with COPD who have cardiovascular disease are at significantly increased risk for COPD exacerbations and increased costs compared with patients with COPD who do not have cardiovascular disease.42 Together, these findings provide strong support for careful monitor-ing of cardiovascular health in patients with COPD.
Osteoporosis. Results from the Third National Health and Nutrition Examination Survey show that risk of osteoporosis increases with disease severity in both men and women with COPD.6 Reduced physical activity and skeletal muscle mass, changes in body composition, and mediators of chronic systemic inflammation (ie, IL-1 and TNF-a) may contribute to the pathogenesis of osteoporosis in patients with COPD.43,44 Risk factors for osteoporosis also may include low vitamin D levels, smoking, increased alcohol intake, genetic factors, and treatment with systemic or inhaled corticosteroids (ICS).44
Corticosteroids are known to reduce calcium absorption, increase calcium excretion, stimulate bone resorption, and reduce bone formation.44 Evidence suggests a strong association between a cumulative prednisone dose of ≥ 1000 mg and reduced bone mineral density (BMD).45 However, studies evaluating the effects of ICS treatment on BMD and osteoporosis have shown inconsistent results.40,46-49 Patients with COPD should be screened for osteopenia, which indicates an increased risk for osteoporosis, and regular monitoring of BMD should be conducted in patients who are receiving intermittent courses of oral corticosteroids or long-term ICS therapy.44
Depression and anxiety. Mood disorders, including depression and anxiety, are more prevalent in patients with COPD than in the general population.20 In a study of 1334 patients with COPD and other chronic breathing disorders, 65% of patients had both depression and anxiety at screening.50 In the Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) observational study, depression requiring treatment was more prevalent in women than men with moderate to very severe COPD (P ≤ .004).51 Moreover, COPD patients with comorbid major depressive disorder or anxiety have higher rates of COPD-related emergency department visits or hospitalizations and health care costs compared with patients with COPD only.52 Other variables associated with depression and anxiety in patients with COPD include physical disability, fatigue, long-term oxygen therapy, low BMI, severe dyspnea, percentage of predicted forced expiratory volume in 1 second < 50%, poor quality of life, presence of comorbidity, living alone, current smoking, and low social class status.53
Depression and anxiety increase the severity of disease symptoms,54 decrease levels of physical activity,20 increase functional impairment,55 and worsen quality of life.20,56,57 In the National Emphysema Treatment Trial (NETT) (N = 610), approximately 41% of patients were mildly to moderately depressed; these patients had a greater 3-year risk of mortality compared with nondepressed patients.58 Anxiety and depressive disorders are underrecognized (< 40%) and undertreated (approximately 30%) in patients with COPD.50 The adverse clinical consequences of anxiety and depression in patients with COPD highlight the need to implement screening procedures and initiate appropriate treatment, such as antidepressants and/or pulmonary rehabilitation.57
Anemia. Putative mechanisms for anemia in chronic diseases include shortened red blood cell survival time, dysregulation of iron homeostasis, and impaired bone marrow erythropoietic response.59 These changes may occur as a result of systemic inflammation involving increased circulating IL-1, TNF-a, interferon-g, and other cytokines and chemokines, supporting a mechanistic link between COPD and anemia.59 Anemia occurs in 13% to 17% of patients with COPD60,61 and is associated with worsening of COPD symptoms, decreased exercise capacity, and greater risk of mortality in patients with COPD.60 Although a causal relationship between COPD and anemia has not been established, findings support screening and appropriate treatment in patients with COPD.60 It should be noted that polycythemia can also occur in patients who have arterial hypoxemia and in continuing smokers, and it is identified by a hematocrit of > 55%.2
EFFECTS OF COMORBIDITIES ON CLINICAL OUTCOMES
Comorbidities of COPD are associated with poor clinical outcomes, although their severity and impact on patient health vary with time and among patients.2 Data from the National Hospital Discharge Survey from 1979 to 2001 indicate that rates of in-hospital mortality due to various cardiovascular, pulmonary, and thoracic conditions are higher in patients with, versus without, COPD.62 COPD currently is the third leading cause of death in adults in the United States63; however, results from several studies suggest that patients with COPD may be more likely to die of comorbid conditions than of COPD,64-66 in particular those related to cardiovascular disease.65,66
THERAPEUTIC IMPLICATIONS
Current Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines recommend that significant comorbidities should be considered during a comprehensive diagnostic assessment of disease sever-ity and determination of appropriate treatment2; however, neither the GOLD guidelines nor the American Thoracic Society/European Res-pi-ratory Society (ATS/ERS) guide-lines give integrated recommendations for management of specific comorbid conditions.2,67 The ATS/ERS guide-lines recommend referral to a special-ist for patients who have cormorbid illness, including osteoporosis, heart failure, bronchiectasis, and lung cancer.67 Considering that 20% of Medicare beneficiaries have ≥ 5 chronic conditions, and half are prescribed
≥ 5 medica-tions for comorbid diseases, it is critical that physicians make efforts to screen for comorbidities and implement disease management programs that consider the “whole patient.”68 The central role of systemic inflammatory process in COPD and its comorbidities supports a need for further research evaluating novel targets for suppression of pulmonary and systemic inflammation, such as phosphodiesterase-4, p38 mitogen–activated protein kinase, and nuclear factor-kB.69
CONCLUSIONS
COPD is associated with chronic airway and systemic inflammation; the latter is a likely mechanism for the many clinically relevant extrapulmonary effects associated with the disease. Systemic comorbidities of COPD may affect multiple physiologic systems and often are associated with poor outcomes in COPD patients. Disease management programs that consider the pulmonary and nonpulmonary effects of COPD and its comorbidities and treat the “whole patient” are critically needed. Research on novel targets for reducing systemic inflammation is also needed in COPD patients with or without existing comorbidities.
Acknowledgments
The author thanks Kristen Quinn, PhD, and Cynthia Gobbel, PhD, from Scientific Connexions (Newtown, PA) who provided medical writing support funded by AstraZeneca LP (Wilmington, DE).
REFERENCES:
1. Agusti AGN. COPD, a multicomponent disease: implications for management. Respir Med. 2005;99:670-682.
2. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. http://www.goldcopd.org. Updated 2010. Accessed May 2, 2011.
3. Agustí AG, Noguera A, Sauleda J, Sala E, Pons J, Busquets X. Systemic effects of chronic obstructive pulmonary disease. Eur Respir J. 2003;21:347-360.
4. Barnes PJ. Chronic obstructive pulmonary disease: effects beyond the lungs. PLoS Med. 2010;7:e1000220. Available at: http://www.plosmedicine.org/article/info%3Adoi%2F10.1371%2Fjournal.pmed.1000220. Accessed October 3, 2011.
5. Sin DD, Man SF. Why are patients with chronic obstructive pulmonary disease at increased risk of cardiovascular diseases? The potential role of systemic inflammation in chronic obstructive pulmonary disease. Circulation. 2003;107:1514-1519.
6. Sin DD, Man JP, Man SF. The risk of osteoporosis in caucasian men and women with obstructive airways disease. Am J Med. 2003;114:10-14.
7. Sin DD, Anthonisen NR, Soriano JB, Agusti AG. Mortality in COPD: role of comorbidities. Eur Respir J. 2006;28:1245-1257.
8. Praticò D, Basili S, Vieri M, Cordova C, Violi F, Fitzgerald GA. Chronic obstructive pulmonary disease is associated with an increase in urinary levels of isoprostane F2alpha-III, an index of oxidant stress. Am J Respir Crit Care Med. 1998;158:1709-1714.
9. Rahman I, Morrison D, Donaldson K, MacNee W. Systemic oxidative stress in asthma, COPD, and smokers. Am J Respir Crit Care Med. 1996;154:
1055-1060.
10. de Jong JW, van der Belt-Gritter B, Koëter GH, Postma DS. Peripheral blood lymphocyte cell subsets in subjects with chronic obstructive pulmonary disease: association with smoking, IgE and lung function. Respir Med. 1997;91:67-76.
11. Noguera A, Busquets X, Sauleda J, Villaverde JM, MacNee W, Agustí AG. Expression of adhesion molecules and G proteins in circulating neutrophils in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1998;158:1664-1668.
12. Noguera A, Batle S, Miralles C, et al. Enhanced neutrophil response in chronic obstructive pulmonary disease. Thorax. 2001;56:432-437.
13. Schols AM, Buurman WA, Staal van den Brekel AJ, Dentener MA, Wouters EF. Evidence for a relation between metabolic derangements and increased levels of inflammatory mediators in a subgroup of patients with chronic obstructive pulmonary disease. Thorax. 1996;51:819-824.
14. Ridker PM. Clinical application of C-reactive protein for cardiovascular disease detection and prevention. Circulation. 2003;107:363-369.
15. Debigaré R, Côté CH, Maltais F. Peripheral muscle wasting in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2001;164:1712-1717.
16. Gan WQ, Man SF, Senthilselvan A, Sin DD. Association between chronic obstructive pulmonary disease and systemic inflammation: a systematic
review and a meta-analysis. Thorax. 2004;59:574-580.
17. Pinto-Plata VM, Müllerova H, Toso JF, et al. C-reactive protein in patients with COPD, control smokers and non-smokers. Thorax. 2006;61:23-28.
18. Franciosi LG, Page CP, Celli BR, et al. Markers of disease severity in chronic obstructive pulmonary disease. Pulm Pharmacol Ther. 2006;19:189-199.
19. Dahl M, Vestbo J, Lange P, Bojesen SE, Tybja´erg-Hansen A, Nordestgaard BG. C-reactive protein as a predictor of prognosis in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2007;175:250-255.
20. Kao CC, Hanania NA. Co-morbidities of COPD: systemic inflammation. In: Crapo J, ed. Atlas of Chronic Obstructive Pulmonary Disease. Philadelphia, PA: Current Medicine Group; 2009:169-177.
21. Walter RE, Wilk JB, Larson MG, et al. Systemic inflammation and COPD: the Framingham Heart Study. Chest. 2008;133:19-25.
22. Mannino DM, Thorn D, Swensen A, Holguin F. Prevalence and outcomes of diabetes, hypertension and cardiovascular disease in COPD. Eur Respir J. 2008;32:962-969.
23. Mapel DW, Hurley JS, Frost FJ, Petersen HV, Picchi MA, Coultas DB. Health care utilization in chronic obstructive pulmonary disease: a case-control study in a health maintenance organization. Arch Intern Med. 2000;160:2653-2658.
24. Chatila WM, Thomashow BM, Minai OA, Criner GJ, Make BJ. Comorbidities in chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2008;5:549-555.
25. van Manen JG, Bindels PJ, IJzermans CJ, van der Zee JS, Bottema BJ, Schadé E. Prevalence ofcomorbidity in patients with a chronic airway obstruction and controls over the age of 40. J Clin Epidemiol. 2001;54:287-293.
26. Soriano JB, Visick GT, Muellerova H, Payvandi N, Hansell AL. Patterns of comorbidities in newly diagnosed COPD and asthma in primary care. Chest. 2005;128:2099-2107.
27. Sidney S, Sorel M, Quesenberry CP Jr, DeLuise C, Lanes S, Eisner MD. COPD and incident cardiovascular disease hospitalizations and mortality: Kaiser Permanente Medical Care Program. Chest. 2005;128:2068-2075.
28. Walsh JW, Thomashow BM. COPD and co-morbidities: treating the whole patient. Results of COPD Foundation national survey. Paper presented at: American Thoracic Society 2006 International Conference; May 19-24, 2006; San Diego, CA.
29. Schols AM, Soeters PB, Dingemans AM, Mostert R, Frantzen PJ, Wouters EF. Prevalence and characteristics of nutritional depletion in patients with stable COPD eligible for pulmonary rehabilitation. Am Rev Respir Dis. 1993;147:1151-1156.
30. Schols AM, Slangen J, Volovics L, Wouters EF. Weight loss is a reversible factor in the prognosis of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1998;157:1791-1797.
31. Agustí AG, Sauleda J, Miralles C, et al. Skeletal muscle apoptosis and weight loss in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2002;166:485-489.
32. Eid AA, Ionescu AA, Nixon LS, et al. Inflammatory response and body composition in chronicobstructive pulmonary disease. Am J Respir Crit Care Med. 2001;164:1414-1418.
33. Sevenoaks MJ, Stockley RA. Chronic obstructive pulmonary disease, inflammation and co-morbidity: a common inflammatory phenotype? Respir Res. 2006;7:70.
34. Balasubramanian VP, Varkey B. Chronic obstructive pulmonary disease: effects beyond the lungs. Curr Opin Pulm Med. 2006;12:106-112.
35. Rennard SI. Clinical approach to patients with chronic obstructive pulmonary disease and cardiovascular disease. Proc Am Thorac Soc. 2005;2:94-100.
36. van Eeden SF, Sin DD. Chronic obstructive pulmonary disease: a chronic systemic inflammatory disease. Respiration. 2008;75:224-238.
37. Curkendall SM, DeLuise C, Jones JK, et al. Cardiovascular disease in patients with chronic obstructive pulmonary disease, Saskatchewan Canada cardiovascular disease in COPD patients. Ann Epidemiol. 2006;16:63-70.
38. Sabit R, Bolton CE, Edwards PH, et al. Arterial stiffness and osteoporosis in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2007;175:1259-1265.
39. Willum-Hansen T, Staessen JA, Torp-Pedersen C, et al. Prognostic value of aortic pulse wave velocity as index of arterial stiffness in the general population. Circulation. 2006;113:664-670.
40. Calverley PM, Anderson JA, Celli B, et al; TORCH investigators. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med. 2007;356:775-789.
41. Rabe KF. Treating COPD: the TORCH trial, P values, and the Dodo. N Engl J Med. 2007;356:851-854.
42. Dalal AA, Shah M, Lunacsek O, Hanania NA. Clinical and economic burden of patients diagnosed with COPD with comorbid cardiovascular disease. Respir Med. 2011;105:1516-1522.
43. Ginaldi L, Di Benedetto MC, De Martinis M. Osteoporosis, inflammation and ageing. Immun Ageing. 2005;2:1-5.
44. Ionescu AA, Schoon E. Osteoporosis in chronic obstructive pulmonary disease. Eur Respir J. 2003;22(suppl):64S-75S.
45. Dubois EF, Röder E, Dekhuijzen PN, Zwinderman AE, Schweitzer DH. Dual energy X-ray absorptiometry outcomes in male COPD patients after treatment with different glucocorticoid regimens. Chest. 2002;121:1456-1463.
46. Ferguson GT, Calverley PMA, Anderson JA, et al. Prevalence and progression of osteoporosis in patients with COPD: results from the TOwards a Revolution in COPD Health study. Chest. 2009;136:1456-1465.
47. Lung Health Study Research Group. Effect of inhaled triamcinolone on the decline in pulmonary function in chronic obstructive pulmonary disease. N Engl J Med. 2000;343:1902-1909.
48. Pauwels RA, Löfdahl CG, Laitinen LA, et al. Long-term treatment with inhaled budesonide in persons with mild chronic obstructive pulmonary disease who continue smoking: European Respiratory Society Study on Chronic Obstructive Pulmonary Disease. N Engl J Med. 1999;340:1948-1953.
49. Rennard SI, Tashkin DP, McElhattan J, et al. Efficacy and tolerability of budesonide/formoterol in one hydrofluoroalkane pressurized metered-dose inhaler in patients with chronic obstructive pulmonary disease: results from a 1-year randomized controlled clinical trial. Drugs. 2009;69:549-565.
50. Kunik ME, Roundy K, Veazey C, et al. Surprisingly high prevalence of anxiety and depression in chronic breathing disorders. Chest. 2005;127:1205-1211.
51. Agusti A, Calverley PM, Celli B, et al. Characterisation of COPD heterogeneity in the ECLIPSE cohort. Respir Res. 2010;11:1-14.
52. Dalal AA, Shah M, Lunacsek O, Hanania NA. Clinical and economic burden of depression/
anxiety in chronic obstructive pulmonary disease patients within a managed care population. COPD. 2011;8:293-299.
53. Maurer J, Rebbapragada V, Borson S, et al; ACCP Workshop Panel on Anxiety and Depression in COPD. Anxiety and depression in COPD: current understanding, unanswered questions, and research needs. Chest. 2008;134(suppl 4):43S-56S.
54. Ng TP, Niti M, Tan WC, Cao Z, Ong KC, Eng P. Depressive symptoms and chronic obstructive pulmonary disease: effect on mortality, hospital readmission, symptom burden, functional status, and quality of life. Arch Intern Med. 2007;167:60-67.
55. Kim HF, Kunik ME, Molinari VA, et al. Functional impairment in COPD patients: the impact of anxiety and depression. Psychosomatics. 2000;41:
465-471.
56. Felker B, Katon W, Hedrick SC, Rasmussen J, McKnight K, McDonnell MB, Fihn SD. The association between depressive symptoms and health
status in patients with chronic pulmonary disease. Gen Hosp Psychiatry. 2001;23:56-61.
57. Norwood R. Prevalence and impact of depression in chronic obstructive pulmonary disease patients. Curr Opin Pulm Med. 2006;12:113-117.
58. Fan VS, Ramsey SD, Giardino ND, et al; National Emphysema Treatment Trial (NETT) Research Group. Sex, depression, and risk of hospitalization and mortality in chronic obstructive pulmonary disease. Arch Intern Med. 2007;167:2345-2353.
59. Similowski T, Agustí A, MacNee W, Schönhofer B. The potential impact of anaemia of chronic disease in COPD. Eur Respir J. 2006;27:390-396.
60. Cote C, Zilberberg MD, Mody SH, Dordelly LJ, Celli B. Haemoglobin level and its clinical impact in a cohort of patients with COPD. Eur Respir J. 2007;29:923-929.
61. John M, Hoernig S, Doehner W, Okonko DD, Witt C, Anker SD. Anemia and inflammation in COPD. Chest. 2005;127:825-829.
62. Holguin F, Folch E, Redd SC, Mannino DM. Comorbidity and mortality in COPD-related hospitalizations in the United States, 1979 to 2001. Chest. 2005;128:2005-2011.
63. Miniño AM, Xu J, Kochanek KD. Deaths: preliminary data for 2008. National Vital Statistics Reports. Hyattsville, MD: Centers for Disease
Control and Prevention, National Center for Health Statistics; 59(2);2010.
64. Anthonisen NR, Connett JE, Enright PL, Manfreda J; Lung Health Study Research Group. Hospitalizations and mortality in the Lung Health Study. Am J Respir Crit Care Med. 2002;166:333-339.
65. Huiart L, Ernst P, Suissa S. Cardiovascular morbidity and mortality in COPD. Chest. 2005;128:
2640-2646.
66. Keistinen T, Tuuponen T, Kivelä SL. Survival experience of the population needing hospital treatment for asthma or COPD at age 50-54 years. Respir Med. 1998;92:568-572.
67. Celli BR, MacNee W; ATS/ERS Task Force. Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper. Eur Respir J. 2004;23:932-946.
68. Tinetti ME, Bogardus ST Jr, Agostini JV. Potential pitfalls of disease-specific guidelines for patients with multiple conditions. N Engl J Med. 2004;351:
2870-2874.
69. Barnes PJ. Future treatments for chronic obstructive pulmonary disease and its comorbidities. Proc Am Thorac Soc. 2008;5:857-864.