
 A 12-year-old girl presents with a 1-year history of itchy lesions on her right leg. The lesions are worse during the winter. She has a history of atopic dermatitis and asthma.
A 12-year-old girl presents with a 1-year history of itchy lesions on her right leg. The lesions are worse during the winter. She has a history of atopic dermatitis and asthma.
The patient has 2 red, raised, coin-shaped lesions: one on the right knee (3.5 cm in diameter) and one on the right shin (6 cm in diameter) (Figure 1). The plaquelike lesions are dry and cracked, with slight scaling. No central pallor is noted. The nails are normal. There is no joint deformity.
Based on the clinical findings and history, nummular eczema is diagnosed.
NUMMULAR ECZEMA: AN OVERVIEWNummular eczema is characterized by coin-shaped eczematous plaques.1 (The word "nummular" is derived from the Latin word nummulus, which means "coinlike.") Synonyms for nummular eczema include discoid eczema, nummular dermatitis, and orbicular eczema.2-4 The condition was first described by Rayer in 1845, and the term was coined by Devergie in 1857.5
Reported prevalence varies widely, from 0.1% to 9%.2 The high rates in some studies may be related to the inclusion of patients with disseminated eczema.2 The condition is rare in the first year of life; thereafter, the incidence increases with age.5,6 Age at onset peaks between 15 and 25 years and again between 55 and 65 years.5 The condition is slightly more common in boys than in girls.2
PATHOGENESIS AND ETIOLOGYThe exact pathogenesis has not been fully elucidated. Neuropeptides substance P, calcitonin gene-related peptide, and mast cells are more frequent in the epidermis and papillary dermis. The increase in neuropeptides substance P and calcitonin gene-related peptide may stimulate keratinocytes to release cytokines, which enhance inflammation. Neurogenic stimulation is maintained by mast cells through activation of neuropeptides substance P and calcitonin gene-related peptide.7
In most cases, the cause is unknown. Some authors report that nummular eczema is more frequent in persons with atopy5; however, serum IgE levels are usually within the normal range.1,8 In one study, 16 (33%) of 48 patients with nummular eczema had at least one clinically relevant positive patch test.9 Nummular eczema may result from contact with nickel, chromate, fragrances, wool, soaps, rubber, or topical medications (neomycin and thioglycolate).1,4,5 Systemic medications, such as isotretinoin(, streptomycin(, isoniazid(, methyldopa(, and the combination of interferon alfa 2b plus ribavirin(, as well as mercury-containing dental alloys, also have been implicated in the pathogenesis.1,5,10-12
Nummular eczema is exacerbated by conditions that promote very dry or xerotic skin--for instance, frequent bathing, low humidity, windy environments, and the winter season.3,8,13 Emotional stress may trigger or exacerbate nummular eczema in susceptible persons.3 Other predisposing factors include alcohol( or tobacco consumption, trauma, venous stasis, and edema of the lower limbs.3,4,9,13 The possibility of bacterial infection as either a direct cause or a hypersensitivity mechanism has not been substantiated.2,5
CLINICAL MANIFESTATIONS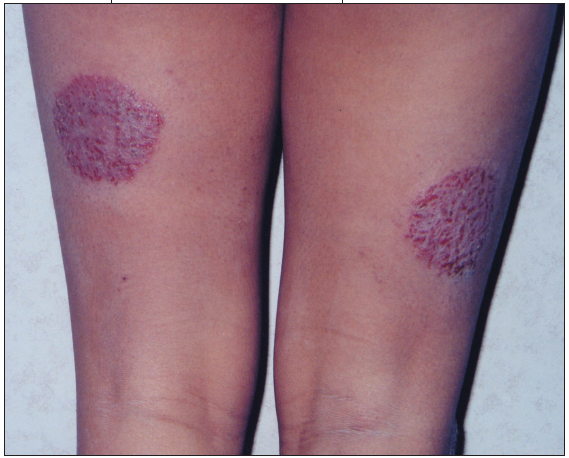 The initial uniform groups of papules and vesicles, with time and itching, become inflamed and may weep.14 The lesions enlarge by confluence or peripheral extension to form the discrete, round or oval, erythematous, scaly, lichenified, hyperkeratotic, hyperpigmented plaques typical of chronic nummular eczema.14 Usually, the lesions are located on the extensor surfaces of the lower extremities and are symmetric (Figure 2).13 The knees, elbows, and scalp are often spared. Itching is moderate to intense. Secondary bacterial infection is common.
The initial uniform groups of papules and vesicles, with time and itching, become inflamed and may weep.14 The lesions enlarge by confluence or peripheral extension to form the discrete, round or oval, erythematous, scaly, lichenified, hyperkeratotic, hyperpigmented plaques typical of chronic nummular eczema.14 Usually, the lesions are located on the extensor surfaces of the lower extremities and are symmetric (Figure 2).13 The knees, elbows, and scalp are often spared. Itching is moderate to intense. Secondary bacterial infection is common.
The course is variable, but usually chronic, and characterized by relapses and remissions.
DIAGNOSISConsider tinea corporis, psoriasis, granuloma annulare, and allergic contact dermatitis in the differential diagnosis:
• Lack of central clearing helps distinguish lesions of nummular eczema from tinea corporis.
• The scales in nummular eczema are thin and sparse, unlike the thick, silvery scales of psoriasis. Pinpoint bleeding after removal of the superficial scales (Auspitz sign), pitting of the nails, and arthropathy suggest psoriasis.
• Granuloma annulare is characterized by necrobiotic dermal papules, which often assume an annular configuration.15 The center is often slightly atrophic or depressed.15
• In allergic contact dermatitis, the site, configuration, and chronicity of the skin lesions are clues to diagnosis. A patch test may confirm the cause.
In nummular eczema, the acute stage is characterized by intercellular edema, intraepidermal vesicles, and perivascular lymphocytic infiltration, and the chronic stage by hyperkeratosis, acanthosis, increase in the granular cell layer, and hyperplasia of the epidermis.5,13
Laboratory tests do not help identify nummular eczema.
MANAGEMENTSuccessful treatment requires avoidance of triggers, optimal skin care, and pharmacotherapy.
Skin care. The following advice can help patients and their parents increase hydration and lubrication of dry skin and minimize itching:
• Improve the ambient humidity and minimize showers or have the child bathe in a tub. Addition of a nonperfumed bath oil to the bath water after a period of soaking might be helpful.
• Apply a nonperfumed moisturizing cream within 3 minutes after the bath to prevent evaporation. The moisturizer should be applied several times a day to all dry skin surfaces. Double applications separated by a few minutes to allow optimal penetration of the cream may be beneficial.
• Keep fingernails manicured and cleansed regularly to minimize trauma and secondary bacterial colonization from scratching. Children who itch overnight may benefit from gloves to prevent further trauma to affected skin.
Pharmacotherapy. Topical corticosteroids result in prompt improvement. Base the potency of the corticosteroid on the severity, site, and extent of the lesions.
Topical immunomodulators, such as tacrolimus( and pimecrolimus(, represent a major new alternative to long-term corticosteroid use, especially in children. These agents are relatively free of side effects and can be safely applied to the entire body.16
Topical antibiotics are indicated for secondary bacterial infection.
OUTCOME OF THE CASEThis patient was provided with instruction on how to lubricate the skin and reduce itching. A topical immunomodulator was prescribed.