
A Boy With a Wheeze: Foreign Body Aspiration Mimicking Asthma
Authors:
Heather B. Minto, MD, and Kelly Maples, MD
A 10-year-old boy presented to an allergy and immunology clinic with an 8-month history of daily wheezing and coughing, as well as significant dyspnea after exercise, resulting in exercise limitation. Previously, the boy had been well, with no history of wheezing, and his current symptoms had not been preceded by an illness or a choking episode.
He had been seen by his pediatrician and was given albuterol for the wheeze but had shown minimal improvement. He then was placed on an inhaled corticosteroid and an oral leukotriene receptor antagonist, but still had no significant improvement. Finally, he completed two 5-day courses of oral corticosteroids; when this measure proved ineffective, chest radiography was done, the results of which were read as normal (Figure 1).

Figure 1. Normal-appearing chest radiograph of a 10-year-old boy with a months-long history of wheeze and cough and significant postexercise dyspnea.
At the age of 5 years, the boy had been hospitalized for right upper-lobe pneumonia, but his past medical history was otherwise negative. He had not had any ear infections, skin infections, or abscesses. He had been growing well, his immunizations were up-to-date, and there was no family history of cystic fibrosis (CF) or primary immunodeficiency.
On physical examination, he was in no distress. He had diminished breath sounds bilaterally, with a significantly prolonged expiratory phase, and scattered expiratory wheezing at both bases. He improved mildly after albuterol nebulizer treatment and 4 puffs of albuterol HFA.
Pulmonary function tests (PFTs) revealed a moderate to severe obstructive pattern without reversibility after a short-acting β-agonist. Forced vital capacity (FVC) was 87% of the predicted value, forced expiratory volume in the first second of expiration (FEV1) was 62% of predicted, midexpiratory phase forced expiratory flow (FEF25%-75%) was 29% of predicted, and FEV1 to FVC ratio was 76% predicted. He was placed on a 14-day regimen of oral corticosteroids, with follow-up scheduled in 2 weeks to assess for spirometric reversibility.
On follow-up examination 2 weeks later, his symptoms had not improved. He still had a wet cough with an expiratory wheeze. Results of PFTs were relatively unchanged, with FEV1 59% of predicted, FVC 71% of predicted, FEF25%-75% 44% of predicted, and FEV1 to FVC ratio 89% of predicted. This clinical picture was concerning for lung pathology other than asthma.
A computed tomography (CT) scan of the chest was ordered, and the boy was referred to a pulmonology consultant for further evaluation.
The pulmonologist ordered laboratory blood testing for α1-antitrypsin deficiency and scheduled a sweat chloride test to screen for CF. (Both tests later would return with negative results.) Sputum culture was positive for Pseudomonas aeruginosa, and the boy was started on a regimen of levofloxacin. The presence of P aeruginosa raised suspicion for CF.
Results of chest CT, performed after pulmonary consultation, showed a foreign body in the right bronchus intermedius (Figure 2).
The boy was referred to an otorhinolaryngologist, who visualized the foreign body via ventilating bronchoscope (Figure 3) and removed the obstruction from the right bronchus intermedius (Figure 4). The foreign body was a round, plastic object with a small amount of granulation tissue deep to it. Otherwise, no obvious injury or deformity was noted.
The patient was seen 2 months later in the pulmonology clinic, and he no longer was coughing or wheezing. His symptoms had completely resolved. PFT results had improved, with FVC 86% of predicted, FEV1 73% of predicted, FEF25%-75% 55% of predicted, and FEV1 to FVC ratio 91% of predicted.
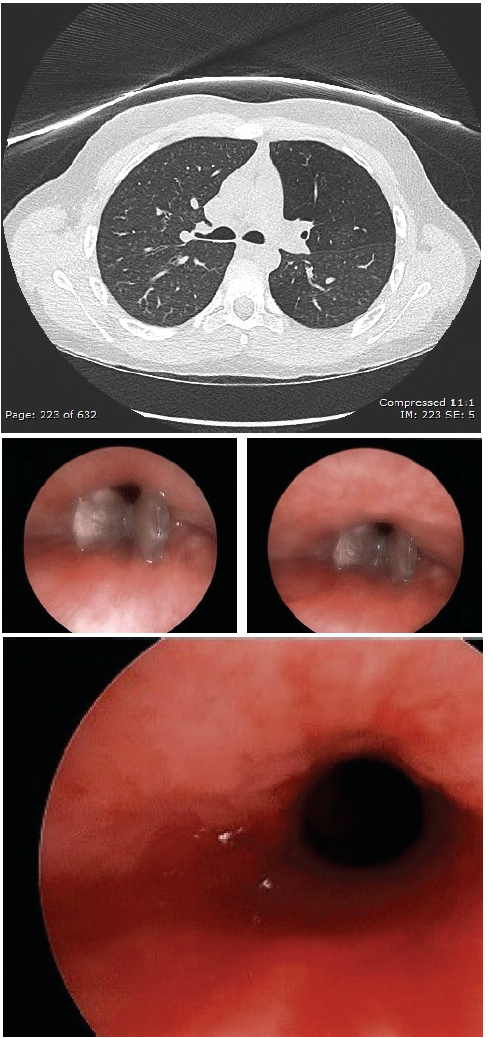
Figure 2. Chest CT image showing a foreign body in the right bronchus intermedius.
Figure 3. Bronchoscopy photographs showing a foreign body in the right bronchus intermedius.
Figure 4. Bronchoscopy photograph after foreign body removal showing a clear right bronchus intermedius.
Differential Diagnosis of Wheezing
The differential diagnosis of wheezing is broad and often is guided by the patient’s age.1 Wheezing results from forceful expulsion of air through narrow airways, and any location along the respiratory tree can be involved. Most commonly, wheezing is attributed to small-airway obstruction.
The list of differential diagnoses (Table) includes asthma, infection (eg, croup, bronchitis, pneumonia), CF, congenital anomaly of the airway (eg, choanal atresia, glottic abnormality, chondromalacia, tracheoesophageal fistula), congenital heart anomaly (eg, double aortic arch, anomalous innominate artery, anomalous left common carotid artery), bronchiolitis obliterans, foreign body aspiration (FBA), vocal cord dysfunction, immunodeficiency, α1-antitrypsin deficiency, and gastroesophageal reflux disease.1

Foreign Body Aspiration
FBA is a common problem in pediatrics. A high index of suspicion is required, because children often present many days after the aspiration episode has occurred. Sometimes a parent may have observed the aspiration or may be concerned that an aspiration may have occurred because an object is missing. Questioning and, often, further testing are needed for patients in whom the symptoms and history are concerning for FBA.
FBA is more common in younger children. Typically, it occurs in children younger then 3 years, who tend to explore their environment by putting objects in their mouth. Also at this time, their sucking, swallowing, and breathing mechanisms are maturing, and they often are mobile, placing them at higher risk of FBA.
Making the diagnosis can be challenging, since many of the symptoms of FBA are nonspecific and are seen with other disease processes. In acute aspiration, symptoms include sudden-onset coughing, choking, and shortness of breath. More often, however, patients present with cough, wheeze, fever, and sometimes dyspnea.
The triad of persistent cough, localized wheezing, and localized decreased breath sounds has been cited as being suggestive of FBA2; however, the absence of clinical symptoms cannot sufficiently exclude FBA in a child with a positive history. The degree of obstruction often correlates with the symptoms experienced, with wheezing often resulting from partial obstruction.
Many authors suggest chest radiography as the first diagnostic test to be considered in cases of suspected FBA.3-5 However, most foreign bodies are not radiopaque but rather are radiolucent and thus do no show up on chest radiographs, as in our patient’s case. Most foreign bodies are food material such as nuts and vegetables, although pebbles, small plastic objects and toys, and small wooden pieces also are commonly aspirated.6 Bronchoscopy is diagnostic, and rigid bronchoscopy is required to remove the foreign body. The decision to perform bronchoscopy is based on history, physical symptoms, and radiography results.7
ASTHMA OR FBA?
Our patient had been previously healthy and had presented to his pediatrician with daily cough and wheezing. Asthma was the initial diagnosis; however, after regimens of albuterol, an inhaled corticosteroid, an oral leukotriene receptor antagonist, and numerous oral corticosteroids, he had gotten no better. Asthma symptoms generally respond to medical therapy; a reversible response to albuterol or systemic corticosteroids is required to make the diagnosis of asthma. A failure to respond to asthma therapy should lead to evaluation for other causes of wheezing.
Although congenital anomalies are potential causes of coughing and wheezing, their presence would be less likely in our patient, since they tend to present in infancy or in early childhood. Still, chest CT was done to evaluate for structural anomalies. When P aeruginosa was isolated from the boy’s sputum culture, significant concern was raised for CF, and a sweat chloride test was performed, which was negative. He also was scheduled for α1-antitrypsin deficiency testing and immunologic testing (again, with negative results), since those would be higher on our list of differential diagnoses given his age.
The plastic foreign body that our patient aspirated was radiolucent and was spotted only on CT images. Further questioning elicited that our patient frequently chewed on plastic pen caps and other small plastic objects. He also is an active boy, which increases his risk of FBA. That the patient did not recall any choking episodes suggestive of aspiration, paired with his age, placed the eventual diagnosis of FBA lower on our initial list of differential diagnoses.
In medicine it can be easy to get fixated on one diagnosis; however, when a patient is not responding to therapy as expected, the differential diagnosis must be broadened. Remember, all that wheezes isn’t asthma.
Heather B. Minto, MD, is a third-year resident in the Department of Pediatrics at Eastern Virginia Medical School and Children’s Hospital of The King’s Daughters in Norfolk, Virginia.
Kelly Maples, MD, is an attending allergist/immunologist at Children’s Hospital of The King’s Daughters.
References
1. Larsen GL, Nichols DP. Functional assessment of asthma. In: Leung DYM, Sampson HA, Geha R, Szefler SJ, eds. Pediatric Allergy: Principles and Practice. 2nd ed. Philadelphia, PA: Mosby Elsevier; 2010:354-362.
2. Louie MC, Bradin S. Foreign body ingestion and aspiration. Pediatr Rev. 2009;30(8):295-301.
3. Howard WA. Differential diagnosis of wheezing in children. Pediatr Rev. 1980;1(8):239-244.
4. Holroyd HJ. Foreign body aspiration: potential cause of coughing and wheezing. Pediatr Rev. 1988;10(2):59-63.
5. Mohan P. Aspiration in infants and children. Pediatr Rev. 2002;23(9):330-331.
6. Midulla F, Guidi R, Barbato A, et al. Foreign body aspiration in children. Pediatr Int. 2005;47(6):663-668.
7. Akelma AZ, Cizmeci MN, Kanburoglu MK, Mete E. An overlooked cause of cough in children: foreign body aspiration. J Pediatr. 2013;163(2):292-293.