
Asthma Control During Pregnancy: Avoiding Frequent Pitfalls
Authors:
Shehabaldin Alqalyoobi, MD; Amir A. Zeki, MD, MAS; and Samuel Louie, MD
Citation:
Alqalyoobi S, Zeki AA, Louie S. Asthma control during pregnancy: avoiding frequent pitfalls. Consultant. 2017;57(11):662-665.
Asthma affects approximately 8.8% of pregnant women in the United States.1 Between 1% and 4% of pregnancies are complicated by poorly controlled asthma. One in 500 expectant mothers experience serious health consequences from uncontrolled asthma during pregnancy, including maternal and/or perinatal death from asphyxia, preeclampsia, intrauterine growth restriction, premature birth, and low birth weight.1
Approximately a third of women experience worsening of their asthma during pregnancy; in another third, asthma severity remains the same; and in the remaining third, asthma severity improves.2,3 The reasons for this variability remain a mystery but may relate to patients’ baseline asthma severity before pregnancy, wherein patients with moderate or severe asthma are expected to experience more acute exacerbations.4 After age 17, women have a 40% higher asthma prevalence than men, experience significantly more asthma attacks, and are hospitalized more often with severe exacerbations.5 Approximately 10% of pregnant women with asthma have an exacerbation during labor.5
Multiple mechanical and hormonal changes affect pulmonary physiology during pregnancy (Table 1). Mucosal and laryngeal edema is common during pregnancy and is partially attributed to the effect of estrogens and placental growth hormone on the mucosa; this leads to rhinosinusitis in approximately 20% of pregnant women.6 Chest wall anatomy is altered due to 40% to 50% increase in the average costal angle (from 68° to 103°). The diaphragm becomes elevated by 4 to 5 cm due to uterine enlargement, but its function remains unaffected.7 Lung function, however, can change due to this diaphragmatic elevation. Functional residual capacity (FRC) is decreased by 18%, or 300 to 500 mL.8 FRC reduction is worse in the supine position, when diaphragmatic elevation is the highest, as a result of increased intra-abdominal pressure.
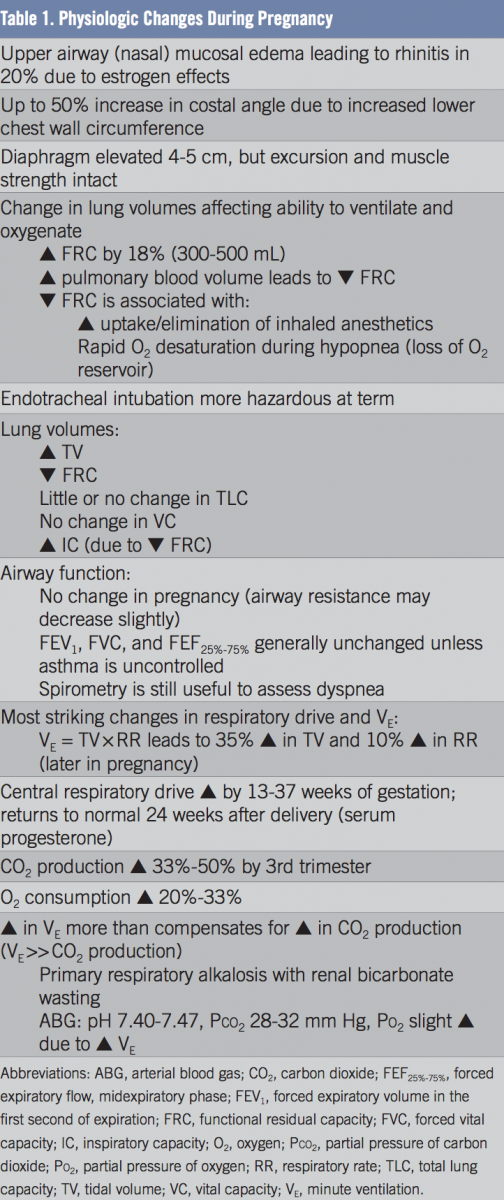
Airway function as measured by forced expiratory volume in the first second of expiration (FEV1) does not change significantly during pregnancy.7 However, minute ventilation and respiratory drive increase significantly. Central drive usually increases by week 13 and continues to week 37, then returns to baseline 6 months after delivery.9 These changes are attributed to the central nervous system effects of progesterone.10 Primary respiratory alkalosis with renal bicarbonate wasting is a normal finding in pregnancy.11 It is attributed to increased minute ventilation that is largely due to a 30% to 40% increase in tidal volume rather than the respiratory rate. Oxygen consumption also increases due to increased maternal and fetal metabolic demands.
NEXT: Diagnostic Considerations During Pregnancy
DIAGNOSTIC CONSIDERATIONS DURING PREGNANCY
Not all that wheezes is asthma, even during pregnancy. Symptoms of asthma are nonspecific and may include episodic cough, dyspnea, wheezing, and chest tightness (Table 2). In our experience, asthma is not often a new diagnosis made during pregnancy. The most common diagnosis other than asthma is dyspnea of pregnancy, which is not typically associated with cough, wheezing, or chest tightness. The differential diagnosis of dyspnea of pregnancy should include gastroesophageal reflux disease (GERD), postnasal drip, edema-related laryngeal and vocal cord dysfunction, occult pulmonary aspiration, hyperventilation, and pulmonary embolism.

Symptoms of asthma peak in the late second or early third trimester, but exacerbations are rare during labor and the peripartum period.12,13 It is important to ask women who are pregnant or planning for pregnancy if they have had a prior asthma diagnosis, so that proper asthma control assessment, management, and medication use can be assured.14
Methacholine challenge testing to rule in or rule out asthma is contraindicated during pregnancy due to the increased risk of triggering acute bronchospasm, resulting in ventilation perfusion mismatching and hypoxemia.15 Pregnancy, nursing, and recent upper respiratory tract infection in the past 2 to 6 weeks are relative contraindications. Absolute contraindications to a methacholine challenge test include an FEV1 less than 50% of predicted or less than 1 L; myocardial infarction or stroke in the past 3 months; uncontrolled hypertension; and aortic aneurysm.
The 2017 Global Initiative for Asthma guidelines consider pregnancy an important risk factor for poor asthma outcomes.15 All pregnant women with asthma should be considered at high risk for frequent exacerbations that can endanger the mother and fetus.16,17 The National Asthma Education and Prevention Program (NAEPP) Working Group on Asthma and Pregnancy recommends that asthma be aggressively treated and managed in pregnant women just as in nonpregnant patients.18,19 At UC Davis, we recommend that all high-risk pregnant women with asthma be referred to asthmatologists who can work with family practitioners and obstetricians in an interdisciplinary fashion to educate and protect the mother and fetus.
Daily use of long-term preventive drug therapies (preferably pregnancy category C or above) to suppress inflammation, in addition to implementation of environmental control measures so that the lowest medication dose is used to control asthma symptoms, reduce impairment and risks to the mother and fetus.
Women with well-controlled mild-to-moderate persistent asthma generally can expect an uncomplicated pregnancy; however, it is essential to identify early on pregnant women with a history of severe persistent asthma or with deteriorating or poorly controlled asthma during the first trimester. These high-risk patients may rely on an albuterol inhaler alone to control symptoms rather than asthma controller medications (eg, inhaled corticosteroids).
High-risk patients may experience socioeconomics-related health care disparities that compromise access to primary care providers and asthma experts. This can lead to poor adherence to controller medications, undermine patient safety, and increase mortality risk.19
ASTHMA CONTROL REQUIRES TEAMWORK
The approach to the high-risk pregnant woman with asthma requires experienced interdisciplinary teamwork from primary care providers, obstetricians, anesthesiologists, nurses, nurse anesthetists, respiratory therapists, and asthmatologists. All persons with previously uncontrolled asthma can benefit from consultation with an asthmatologist.
The keys to successful asthma management during pregnancy are no different than for the nonpregnant patient with asthma. Explain to every patient the concept of asthma control to reduce impairment and reduce risks from asthma exacerbations and drug adverse effects. Frequent assessment of asthma control is needed during pregnancy and can be done readily, for example, with the Asthma Control Test,20 which is available in many languages.
Patient education is absolutely essential to help patients recognize poorly controlled asthma and acute exacerbations early. Proper patient self-management with asthma controller medications in a written asthma action plan with access to clinicians for questions and guidance during pregnancy promotes patient safety and can reduce anxiety. The correct use of a rescue albuterol inhaler for breakthrough symptoms is absolutely essential. At UC Davis, we ask all pregnant patients with asthma how quickly they experience relief from the use of their albuterol inhaler; if the answer is greater than 1 to 2 minutes, clinicians and asthmatologists must recognize the need to educate and train patients on the correct use of albuterol inhalers.
PHARMACOTHERAPY OPTIONS
While the 2007 NAEPP asthma guidelines19 are overdue for revision, major changes are not anticipated, except for the introduction of the long-acting muscarinic-receptor antagonist tiotropium and defining the role of new biologics other than omalizumab. The NAEPP guidelines offer 6 stepwise recommendations to guide clinicians in the prescription of asthma controllers.
Step 1. Preferred: short-acting β2-agonist.
Step 2. Preferred: low-dose inhaled corticosteroid (ICS); alternative: leukotriene-receptor antagonist (LTRA), nedocromil, theophylline.
Step 3. Preferred: low-dose ICS plus long-acting β2-agonist (LABA), or medium-dose ICS; alternative: low-dose ICS plus LTRA, theophylline, or zileuton.
Step 4. Preferred: medium-dose ICS plus LABA; alternative: medium-dose ICS plus LTRA, theophylline, or zileuton. Referral to an asthmatologist is recommended beginning at Step 4.
Step 5. Preferred: high-dose ICS plus LABA; consider omalizumab injection.
Step 6. Preferred: high-dose ICS plus LABA plus oral corticosteroid; consider omalizumab injection.
All pregnant patients with asthma at UC Davis Asthma Network clinics are warned about the boxed warning from the Food and Drug Administration (FDA) stating that LABAs and LABA-containing drugs increase asthma deaths. Patients should thoroughly understand this if LABA-containing medication is prescribed, and the conversation should be documented in the electronic medical record. Safety never happens by accident. We also recommend against stepping down controller treatment until after delivery.15
The fraction of exhaled nitric oxide (FeNO) is elevated in pregnant women with asthma compared with those without asthma and correlates with the level of asthma control.21 Asthma exacerbations during pregnancy may be reduced by monitoring FeNO. In a study of pregnant, nonsmoking women with asthma, Powell and colleagues found that stepping up asthma therapy when the FeNO was greater than 29 ppb and stepping down therapy when the FeNO was less than 16 ppb improved asthma outcomes.22 The currently accepted reference range for FeNO is less than 25 ppb, but there is speculation that an FeNO level greater than 40 ppb may indicate poorly controlled asthma, presumably from active eosinophilic airway inflammation.
It is always concerning to begin or add a new medication for uncontrolled asthma during pregnancy. However, in our opinion, uncontrolled asthma is a far greater risk to the expectant mother and fetus than any known risk from asthma medications.
Most of the adverse effects of asthma medications in pregnancy have been extrapolated from animal studies.23 The FDA is phasing out pregnancy categories A, B, C, D, and X,24 but we still find them helpful in answering the questions expectant parents ask about birth defects. Nevertheless, it is important to evaluate the risks, benefits, and safety of each medication and any interaction with other medications and discuss this with the patient before prescribing.25
SMOKING AND OTHER COMORBIDITIES
It is obviously important to assess the pregnant woman’s readiness to quit smoking or consuming tobacco products without the use of nicotine-replacement products, and refer her urgently to a smoking-cessation program. Nicotine replacement is associated with an increased risk of low-birth-weight and an increased risk of not carrying to term. Varenicline and bupropion are in pregnancy category C.
Treatment of comorbidities that may complicate asthma, such as allergic rhinitis, sinusitis, and GERD, is another important aspect of asthma management. Proton-pump inhibitors are in category B, except for omeprazole. All H2-receptor blockers are in category B. The antihistamines cetirizine, loratadine, and levocetirizine are in category B, whereas fexofenadine and desloratadine are in category C. Azelastine is category C. Montelukast is in category B and zileuton in category C. Budesonide is in category B, and all other inhaled and intranasal ICSs are in category C, with the exception of inhaled triamcinolone, which is in category D and should be avoided. Epinephrine also is in category D.
Ergonovine and prostaglandin F2α, used to treat uterine atony after childbirth, precipitate bronchospasm and must be avoided in women with asthma.
Administration of the inactivated influenza vaccine is recommended during the second and third trimesters if pregnancy coincides with peak influenza outbreaks. The best time to administer the influenza vaccine is during October and November. It is inadvisable to give the inactivated influenza vaccine in women with a history of a serious prior reaction or egg allergy. The intranasal, live attenuated influenza vaccine is contraindicated in pregnant women.
The most common mistake made by health care professionals and/or expectant parents is to delay regularly scheduled primary care assessment of asthma control and treatment for very poorly controlled asthma. This leads to an to an underestimation of asthma severity and an overestimation of asthma control during pregnancy, a lack of appropriate environmental control measures, the undertreatment of chronic persistent asthma symptoms, and the delay of potentially lifesaving treatment during acute severe exacerbations.

Shehabaldin Alqalyoobi, MD, is a fellow in the Department of Internal Medicine, Division of Pulmonary, Critical Care, and Sleep Medicine, at UC Davis Medical Center in Sacramento, California.
Amir A. Zeki, MD, MAS, is an assistant professor in the Department of Internal Medicine, Division of Pulmonary, Critical Care, and Sleep Medicine, and codirector of the UC Davis Asthma Network at UC Davis Medical Center in Sacramento, California.
Samuel Louie, MD, is a professor of medicine in the Department of Internal Medicine, Division of Pulmonary, Critical Care, and Sleep Medicine, and director of the ROAD Center at UC Davis Medical Center in Sacramento, California.
References:
- Kwon HL, Triche EW, Belanger K, Bracken MB. The epidemiology of asthma during pregnancy: prevalence, diagnosis, and symptoms. Immunol Allergy Clin North Am. 2006;26(1):29-62.
- Gluck JC, Gluck PA. The effect of pregnancy on the course of asthma. Immunol Allergy Clin North Am. 2006;26(1):63-80.
- McCallister JW. Asthma in pregnancy: management strategies. Curr Opin Pulm Med. 2013;19(1):13-17.
- Belanger K, Hellenbrand ME, Holford TR, Bracken M. Effect of pregnancy on maternal asthma symptoms and medication use. Obstet Gynecol. 2010;115(3):559-567.
- Schatz M, Dombrowski MP. Asthma in pregnancy. N Engl J Med. 2009;360(18):1862-1869.
- Ellegård EK. Clinical and pathogenetic characteristics of pregnancy rhinitis. Clin Rev Allergy Immunol. 2004;26(3):149-159.
- Weinberger SE, Weiss ST, Cohen WR, Weiss JW, Johnson TS. Pregnancy and the lung. Am Rev Respir Dis. 1980;121(3):559-581.
- Cugell DW, Frank NR, Gaensler EA, Badger TL. Pulmonary function in pregnancy. I. Serial observations in normal women. Am Rev Tuberc. 1953;67(5):568-597.
- Contreras G, Gutiérrez M, Beroíza T, et al. Ventilatory drive and respiratory muscle function in pregnancy. Am Rev Respir Dis. 1991;144(4):837-841.
- Skatrud JB, Dempsey JA, Kaiser DG. Ventilatory response to medroxyprogesterone acetate in normal subjects: time course and mechanism. J Appl Physiol. 1978;44(6):939-944.
- Lucius H, Gahlenbeck H, Kleine HO, Fabel H, Bartels H. Respiratory functions, buffer system, and electrolyte concentrations of blood during human pregnancy. Respir Physiol. 1970;9(3):311-317.
- Elsayegh D, Shapiro JM. Management of the obstetric patient with status asthmaticus. J Intensive Care Med. 2008;23(6):396-402.
- Mabie WC, Barton JR, Wasserstrum N, Sibai BM. Clinical observations on asthma in pregnancy. J Matern Fetal Med. 1992;1(1):45-50.
- Murphy VE, Gibson PG. Asthma in pregnancy. Clin Chest Med. 2011;32(1):93-110.
- Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention, 2017. http://ginasthma.org/2017-gina-report-global-strategy-for-asthma-management-and-prevention. Accessed October 16, 2017.
- Murphy VE, Clifton VL, Gibson PG. Asthma exacerbations during pregnancy: incidence and association with adverse pregnancy outcomes. Thorax. 2006;61(2):169-176.
- Maselli DJ, Adams SG, Peters JI, Levine SM. Management of asthma during pregnancy. Ther Adv Respir Dis. 2013;7(2):87-100.
- National Asthma Education and Prevention Program, Asthma and Pregnancy Working Group. NAEPP Expert Panel report: managing asthma during pregnancy: recommendations for pharmacologic treatment—2004 update. J Allergy Clin Immunol. 2005;115(1):34-46.
- National Asthma Education and Prevention Program. Expert Panel Report 3 Summary Report 2007: Guidelines for the Diagnosis and Management of Asthma. Bethesda, MD: National Institutes of Health; 2007. NIH publication 08-5846. https://www.nhlbi.nih.gov/files/docs/guidelines/asthsumm.pdf. Published October 2007. Accessed October 16, 2017.
- Asthma Control Test™. Asthma.com. http://www.asthma.com/additional-resources/asthma-control-test.html. Published January 2017. Accessed October 16, 2017.
- Tamási L, Bohács A, Horváth I, Losonczy G. Asthma in pregnancy—from immunology to clinical management. Multidiscip Respir Med. 2010;5(4):259-263.
- Powell H, Murphy VE, Taylor DR, et al. Management of asthma in pregnancy guided by measurement of fraction of exhaled nitric oxide: a double-blind, randomised controlled trial. Lancet. 2011;378(9795):983-990.
- Vasilakis-Scaramozza C, Aschengrau A, Cabral HJ, Jick SS. Asthma drugs and the risk of congenital anomalies. Pharmacotherapy. 2013;33(4):363-368.
- US Food and Drug Administration. Summary of proposed rule on pregnancy and lactation labeling. http://www.fda.gov/Drugs/DevelopmentApprovalProcess/DevelopmentResources/Labeling/ucm093310.htm. Updated December 3, 2014. Accessed October 16, 2017.
- Chan AL, Juarez MM, Gidwani N, Albertson TE. Management of critical asthma syndrome during pregnancy. Clin Rev Allergy Immunol. 2015;48(1):45-53.