
Assistive Devices for Independence in the Elderly: A Case Series
Key words: Activities of daily living, assistive devices of independence, functional impairment, assistive device reimbursement.
__________________________________________________________________________________________
One in five Americans will be elderly by the year 2050, and the “oldest old” age group—those defined as 85 years and older—is projected to increase from 3 million in 1994 to 19 million in 2050, accounting for up to 5% of the total US population at that time.1 This older age group comprises the heaviest users of long-term care.
An association between geriatric syndromes and dependency in activities of daily living (ADLs) has been documented by the Health and Retirement Study.2 Poor functional status also has been shown to increase the rate of hospitalization and nursing home placement.3 Thus, the role of geriatricians and other physicians who care for elders should include functional evaluations aimed at improving the overall quality of life for these patients. Carefully selected assistive devices for independence (ADIs) can improve and sometimes modify functional impairment in elderly persons, reducing the risk of falls and their associated financial burdens, while also reducing the costs of disability.4-6
ADIs are classified as specific for ambulation and mobility, for ADLs, and for safety, hearing, and vision.7 While these devices have become more widely accepted, often professional assistance is not sought during their selection.8,9 This case series examines ADIs for elders and highlights the importance of their use by physicians and other providers who care for elderly persons in various healthcare settings.
Case 1
A 73-year-old man with a seizure disorder was functional at home until he developed gradual onset of dizziness, confusion, ataxia, and falls requiring several acute hospitalizations within a 2-month timeframe. His medication list included phenytoin for seizures and meclizine for dizziness. A diagnosis of phenytoin toxicity was made based on his serum phenytoin level of 35 mg/L (normal range, 10 to 20 mg/L). His electroencephalogram suggested generalized slowing with disorganized electrical background activity, but there were no focal or lateralizing discharges. The results of his carotid Doppler ultrasonography, transthoracic echocardiography, brain magnetic resonance imaging, and magnetic resonance angiography were normal. Cerebrospinal fluid analysis demonstrated no abnormalities.
On physical examination, the patient’s gait was unsteady and he had difficulty with transfers. He required setup assistance for meals and self-care, but he did not require hearing or visual aids. Phenytoin was discontinued, and he was started on levetiracetam by the neurologist. Physical therapy was consulted for debility. Although barriers to his therapy included dizziness, delirium, polypharmacy, and an adverse drug reaction to phenytoin, his balance, transfer abilities, and endurance improved with physical therapy, enabling him to achieve a set goal of walking 250 feet with a walker. His family was advised regarding fall prevention. Nonskid footwear and the use of a nightlight were recommended. His daughter was also willing to move closer to be more involved in his care.
The patient’s functional status improved, and he had no more reported falls with the use of a walker. His confusion and ataxia also resolved. He was discharged from the hospital to his home after 1 week of hospitalization, with outpatient physical therapy and support from home health aides. A front-wheeled walker and a bedside commode were prescribed. He was also advised to follow up with a neurologist as an outpatient.
Case 2
A 60-year-old man with chronic hip and knee pain from degenerative joint disease who ambulated with a single-point cane was admitted to the nursing home after sustaining a stroke, which resulted in residual right hemiparesis. The patient’s set goal was to return to baseline function at discharge from the nursing home. Table 1 summarizes the functional course of this patient during therapy. Despite hip and knee pain being a barrier to therapy, treatment with an analgesic and physical therapy enabled him to achieve modified independent ambulation using a front-wheeled walker. His abilities to perform ADLs also improved with the prescribed ADIs. He was discharged to his home after 9 months in the nursing home, with orders for home health aides and physical therapy. A tub-transfer bench, an extended long-handled sponge, a bedside commode with arms, a long-handled shoehorn, and sock aids were also prescribed.

Case 3
A 77-year-old man with medical comorbidities, including diabetes, hypertension, morbid obesity, coronary artery disease, osteoarthritis of the left shoulder, depression, chronic obstructive pulmonary disease, hearing impairment requiring hearing aids, and essential tremors lived at home with his wife and initially ambulated with a cane, but had transitioned to a front-wheeled walker as his gait instability worsened. The patient required a right below-the-knee amputation for peripheral vascular disease and was discharged to his home following rehabilitation in a skilled nursing facility. He required only minimal assistance for most ADLs and could independently operate a powered wheelchair. There was a ramp at the rear entrance of his home. He also had a shower tub, nonskid bath mats, and two grab bars in his bathroom.
Approximately 10 months later, he had a left below-the-knee amputation for osteomyelitis and was readmitted to the nursing home. During his stay at the nursing home, he experienced numerous complications and barriers to recovery, including pressure ulcers, pneumonia, pulmonary embolism, and worsening depression related to the death of another resident in the facility. His goals of care were to eliminate his left lower extremity pain and to improve his ability to perform his ADLs, which were affected by his tremors. Weighted utensils were tried to reduce his tremors during feeding, but without success. Table 2 summarizes the functional course of this patient during therapy.

Although the patient had no measurable improvement with rehabilitation therapy and remained a nursing home resident, several ADIs improved his quality of life in this setting. He was prescribed a power mobility device with a tilt and recline system to assist with mobilization, and his hearing aids remained invaluable in addressing his hearing impairment.
Discussion
The International Classification of Functioning, Disability, and Health is a framework of the World Health Organization (WHO) that describes the concept of health and disability.10 This WHO concept takes into account the complex interactive factors (ie, pathophysiological, psychological, and socioeconomic) that affect overall functioning in elders, and is useful for application to the geriatric setting. About half of US adults 65 years and older have at least one geriatric syndrome in addition to other prevalent chronic medical comorbidities.2 ADIs are mostly used by adults in this age group.11 Older adults with functional impairment may ameliorate their disabilities with appropriately selected ADIs and disease-appropriate medical, surgical, and physical rehabilitation interventions.
The provision of geriatric services designed to manage functional impairment and associated medical cormobidities can result in favorable outcomes, including lower hospitalization rates and significant healthcare cost savings related to disability and nursing home placement.12 Although ADIs for ambulation are described as “the cornerstone in maintaining functionality in persons with temporary or permanent disability,”13 maintaining functionality in elders would be optimally achieved through a coordinated multidisciplinary approach involving physicians, physiatrists, physical and occupational therapists, social workers, and case managers.
The physicians’ role should include proper documentation and prognostication of underlying diagnoses and insight on the intended goals of the prescribed ADI. The physician may also be required to generate a letter of medical necessity. Physiatrists are physicians trained in physical and rehabilitation medicine, and they can play a pivotal role in the evaluation and management of physical impairments. Physical therapists are valuable in implementing the set goals of rehabilitation. They provide patient education on device operability and on the implications of improperly using these devices. The following section explains several types of available ADIs.
ADIs for Ambulation and Mobility
ADIs for ambulation provide stability, reduction of weight-bearing load, and augmentation of muscle action.13 Devices for impaired ambulation include canes, hemi-walkers, walkers, and crutches, while devices for impaired mobility include wheelchairs and power-operated vehicles.14
A cane is useful when only one upper extremity is needed for balance or to bear weight.15 Canes should be held on the hand of the unaffected side to reduce the force needed to support bodyweight.16,17 This helps decrease the force generated across the affected hip joint, thereby decreasing the work of the gluteus muscles. Holding a cane on the impaired side during ambulation increases the workload of the affected hip to the point that it is supporting up to four times the patient’s bodyweight.18
Determining the proper cane length is important for accommodating an individual’s height and support needs. Depending on the type of cane used, up to 25% of bodyweight can be unloaded, and incorrectly fitted canes produce an inefficient gait.7,19 Single-point canes are used for mildly impaired stability, whereas quad canes are useful for weight bearing and sometimes in cases of moderately impaired stability. Ortho canes provide better grip and more controlled balance. These canes are suitable for patients with painful gait disorders, such as osteoarthritis.7 White canes are often used by people who are blind or visually impaired, and their use can help others to identify these patients.
A hemi-walker, also known as a “walk cane,” provides more balance than a quad cane. It is a suitable device for moderate to severe unilateral weakness or hemiplegia. Unlike a quad cane with four legs, the hemi-walker has a vertical component with a handle with two legs and also has two additional legs away from the patient.13
Walkers provide maximum support and balance. They are often indicated when both upper extremities are needed for weight bearing or the patient has bilateral lower-extremity weakness.7 Walkers can be placed along a spectrum of stability at one end and maneuverability at the other. The standard walker is also called a “pick-up walker.” It provides stability and balance but has limited maneuverability. This type of walker has no wheels and is suitable for patients who cannot bear much weight but have the cognitive ability to coordinate the device.
The front-wheeled walker, or the “rolling walker,” provides some degree of stability and maneuverability. It is suited for individuals with a faster gait than that required with a pick-up walker and is useful for individuals with the limited strength to lift a pick-up walker. The four-wheeled walker, often called a “rollator,” provides the most maneuverability with minimal energy, but affords the least balance and stability. Four-wheeled walkers are suitable for people who do not necessarily require a device to bear weight, but who need a large base for support.13,20 A specific type of four-wheeled walker that features a seating platform for rest, a carrying basket, and a handbrake device is commonly used by patients with poor cardiac or pulmonary reserves or by patients with poor endurance.
Crutches are less commonly used for geriatric patients because they require a significant amount of coordination and upper body strength. A single crutch, however, when used by patients who can properly manage it, can offset up to 80% of bodyweight.21
Mobility aids, wheelchairs, and power-operated vehicles are used when ambulation is not feasible because of permanent or temporary impairment. They improve mobility, positioning, and support for some individuals.22 In general, wheelchairs are either manual or powered. Powered wheelchairs and other power-operated vehicles are called power mobility devices (PMDs). In general, PMDs are not recommended for cognitively impaired individuals, and manual wheelchairs are not recommended for those with bilateral impairment of the upper extremities. It is paramount that all wheelchairs have quality seat cushions to prevent pressure ulcer formation. Home modifications are often required to accommodate wheelchairs, including widened doorways, car lifts, and ramps.
Prescribing a wheelchair and its accessories, as with other ADIs, should be tailored to individual needs. For example, an arm trough would be useful for an individual with quadriplegia, hemiplegia, or uncontrolled arm movement. A tilt system allows for changes in the seat orientation in relationship to the ground and recline systems allow changes in seat-to-back angle orientation.23 The tilt and recline system is ideal for patient in prolonged static positions because it can reduce pain and the risk of pressure ulcers.
Devices for transfer can also aid ambulation and mobility. These devices include gait belts, transfer boards, and lifts. Gait belts are also called walking belts. They assist in the safe transfer and ambulation of patients while preventing caregiver back injuries. They are available in various sizes to accommodate different weights. Transfer boards and patient lifts promote easier transfers and repositioning from a wheelchair, bed, chair, or commode. Stand-assist lifts aid walking and weight-bearing, whereas bedside lifts assist with easy transfers from beds to other resting places.7 Trapeze bars are useful for bed positioning and for getting in and out of bed when there are mobility limitations from respiratory diseases or other medical disorders.
ADIs for Hearing, Vision, and ADLs
Hearing aids and vision aids like glasses are important ADIs for enhancing independence, as hearing and sight are essential for performing many ADLs and for maximizing use of other ADIs. In addition to hearing and sight, limited hand function, reduced range of motion, poor fine-motor control, or poor coordination can impair a person’s ability to perform ADLs, impeding their independence. In such persons, certain ADIs can help improve ADL function and self-care, including built-up utensils, universal cuffs with utensil holders, plate guards, rocker knives, and weighed utensils for eating. Reachers and grabbers are useful for individuals with impaired range of motion in the shoulder or for those who have proximal weakness. These devices are designed to help grasp items from hard-to-reach places with minimal stretching or bending, activities that can result in injuries. Devices that enhance dressing include button and zipper hooks, fabric hook-and-loop fasteners, elastic shoelaces, sock aids, and long-handled shoehorns.
Devices that assist with self-care also promote safety by reducing the risk of falls and other injuries among persons with gait instability. The bathroom is an area where safety is a major concern, but there are many ADIs that can be used in this area to reduce safety risks. Toileting ADIs include raised toilet seats and grab bars. Persons who are unable to ambulate to a bathroom can use toilet chairs and bedside or rolling commodes. ADIs for bathing include tub-transfer benches, handheld showers, grab bars on tubs or showers, shower chairs, and nonskid bath mats. Wash mitts and long-handled sponges can be used to ease bathing tasks, whereas built-up combs and brushes, electric toothbrushes, and electric razors with custom handles can facilitate grooming.7
Medicare Reimbursement Guidelines for ADIs
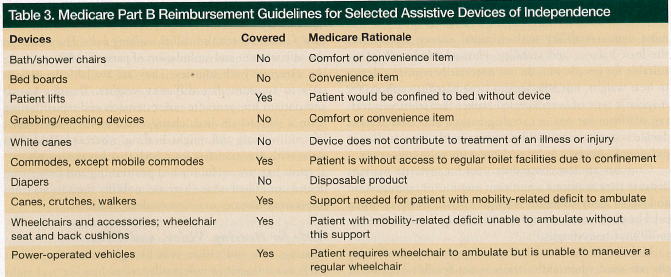
Affordability is an important factor in the selection of ADIs; thus, providers who care for elders should be aware of Medicare’s reimbursement guidelines.24 Medical items that are covered by Medicare require a physician’s prescription. Under Medicare guidelines, durable medical equipment (DME) includes, but is not limited to, canes, walkers, wheelchairs, commode chairs, and lifts. DME is defined as medically necessary, long-lasting equipment prescribed for home use. Costs are covered under Medicare Part B, although patients may be expected to cover some of the cost. Details of out-of-pocket expenses can be obtained from a DME regional carrier. Comfort, convenience, or self-help devices are considered nonmedical and are not paid for by Medicare. Table 3 summarizes the Medicare reimbursement guidelines for some DME.
Medicare will not pay for hearing aids; however, it will reimburse for an audiology examination if prescribed by a physician. Medicare also does not cover routine dental care or most dental procedures, including dentures. Eyeglasses or contact lenses are not routinely paid for; however, these visual aids would be reimbursed for patients who have undergone cataract surgery or implantation of an intraocular lens.
Conclusion
ADIs are vital for enhancing independence in functionally impaired elders. The goal of regaining and maintaining optimal independence is often achieved by using carefully selected ADIs and initiating appropriate disease-specific interventions, as illustrated by case 1 in this report. When this goal is not attainable, modified independence may still be achieved, as illustrated by case 2. Some patients are ultimately unable to attain enough improvement with rehabilitation therapy to regain independence and require long-term care services, but the use of specific ADIs by these patients may still improve their quality of life within their disease-imposed limitations, as illustrated by case 3.
Functional recovery in elderly persons may be affected by many barriers, including polypharmacy, adverse drug reactions, pain, depression, delirium, and medical comorbidities. Therefore, to regain and maintain functional independence, a multidisciplinary approach is optimal. Studies have shown this approach to improve outcomes, leading to reductions in hospitalization rates and disability-related costs. Because ADIs can be essential in helping patients optimize functional independence and maximize their safety and quality of life, it is imperative for all healthcare providers caring for elderly persons to become familiar with ADIs and their uses. To meet the ever-changing needs of geriatric patients, medical and functional evaluations and reassessments of therapeutic strategies, including of ADIs, should be carried out periodically, irrespective of the care setting.
References
- US Census Bureau. Sixty-five Plus in the United States: Statistical Brief. Washington, DC: US Census Bureau; May 1995. [Changes per AMA style, p 57]
- Cigolle CT, Langa KM, Kabeto MU, et al. Geriatric conditions and disability: the Health and Retirement study. Ann Intern Med. 2007;147(3):156-164.
- Crooks V, Waller S, Smith T, Hahn TJ. The use of the Karnofsky Performance Scale in determining outcomes and risk in geriatric outpatients. J Gerontol. 1991;46(4):M139-M144.
- Joyce BM, Kirby RL. Canes, crutches and walkers. Am Fam Physician. 1991;43(2):535-542.
- Bateni H, Maki BE. Assistive devices for balance and mobility: benefits, demands, and adverse consequences. Arch Phys Med Rehabil. 2005;86(1):134-145.
- Verbrugge LM, Rennert C, Madans JH. The greater efficacy of personal and equipment assistance in reducing disability. Am J Public Health. 1997;87(3):384-392.
- Kedlaya D, Kuang T. Assistive devices to improve independence. Medscape Reference. http://emedicine.medscape.com/article/325247-overview. Published June 2011. Accessed June 14, 2012.
- Kuan TS, Tsou JY, Su FC. Hemiplegic gait of stroke patients: the effect of using a cane. Arch Phys Med Rehabil. 1999;80(7):777-784.
- Mann WC, Ottenbacher KJ, Fraas L, Tomita M, Granger CV. Effectiveness of assistive technology and environmental interventions in maintaining independence and reducing home care costs for frail elderly: a randomized controlled trial. Arch Fam Med. 1999;8(3):210-217.
- World Health Organization. International Classification of Functioning, Disability and Health: ICF. Geneva, Switzerland: World Health Organization; 2001. http://www.who.int/classifications/icf/en/. Accessed June 14, 2012.
- Alexander NB. Gait disorders in older adults. J Am Geriatr Soc. 1996;44(4):434-451.
- Barrett DL, Secic M, Borowske D. The gatekeeper program: proactive identification and case management of at-risk older adults prevents nursing home placement, saving healthcare dollars program evaluation. Home Healthc Nurse. 2010;28(3):191-197.
- Faruqui S, Jaeblon T. Ambulatory assistive devices in orthopaedics: uses and modifications. J Am Acad Orthop Surg. 2010;18(1):41-50.
- Dicianno BE, Tovey E. Power mobility device provision: understanding Medicare guidelines and advocating for clients. Arch Phys Med Rehabil. 2007;88(6):807-816.
- Van Hook FW, Demonbreun D, Weiss BD. Ambulatory devices for chronic gait disorder in the elderly. Am Fam Physician. 2003;67(8):1717-1724.
- Jebsen RH. Use and abuse of ambulation aids. JAMA. 1967;199:5-10.
- Blount WP. Don’t throw away the cane. J Bone Joint Surg Am. 1956;38-A(3):695-708.
- Deathe AB, Hayes KC, Winter DA. The biomechanics of canes, crutches, and walkers. Crit Rev Phys Rehab Med. 1993;5:15-29.
- Milczarek JJ, Kirby RL, Harrison ER, MacLeod DA. Standard and four-footed canes: their effect on the standing balance of patients with hemiparesis. Arch Phys Med Rehabil. 1993;74(3):281-285.
- Goldberg B, Hsu JD. Atlas of Orthoses and Assistive Devices. 3rd ed. Philadelphia, PA: Mosby, 1997:557-573.
- Shoup TE, Fletcher LS, Merrill BR. Biomechanics of crutch locomotion. J Biomech. 1974;7:11-19.
- Requejo PS, Kerdanyan G, Minkel J, Adkins R, Walters R. Effect of rear suspension and speed on seat forces and head accelerations experienced by manual wheelchair riders with spinal cord injury. J Rehabil Res Dev. 2008;45(7):985-96.
- Dicianno BE, Arva J, Lieberman JM, Schmeler MR; Rehabilitation Engineering & Assistive Technology Society of North America. RESNA Position on the Application of Tilt, Recline and Elevation of Legrests for Wheelchairs. http://bit.ly/KXM9WA. Published April 2008. Accessed June 14, 2012.
US Centers for Medicare & Medicaid Services. Your Medicare coverage. www.medicare.gov/coverage/. Accessed June 14, 2012.
Disclosure:
The author reports no relevant financial relationships.
Address correspondence to:
Omotayo M. Olatinwo, MD
St. Frances Cabrini Hospital
3330 Masonic Drive
Alexandria, LA 71301
tolatinwo2001@yahoo.com