
Hypertension in a Toddler With Bell Palsy
Case In Point
An Intriguing Diagnosis
 A 22-month-old boy was brought to the emergency department for evaluation of poor appetite, vomiting, and subjective weight loss of 3 months’ duration. He had no fever, diarrhea, abdominal pain, or change in activity. Two months earlier, idiopathic Bell palsy was diagnosed and treatment with oral corticosteroids was started. However, the child’s symptoms persisted. One month before presentation, he was evaluated at another hospital and treated for dehydration. Laboratory results at that time were notable for hypokalemia and hyponatremia. He was given an oral potassium supplement and discharged home.
A 22-month-old boy was brought to the emergency department for evaluation of poor appetite, vomiting, and subjective weight loss of 3 months’ duration. He had no fever, diarrhea, abdominal pain, or change in activity. Two months earlier, idiopathic Bell palsy was diagnosed and treatment with oral corticosteroids was started. However, the child’s symptoms persisted. One month before presentation, he was evaluated at another hospital and treated for dehydration. Laboratory results at that time were notable for hypokalemia and hyponatremia. He was given an oral potassium supplement and discharged home.
The child’s perinatal course was unremarkable. There was no family history of hypertension.
The patient was fussy but consolable. He had left lower facial weakness, consistent with Bell palsy (Figure 1). His height and weight were normal. Temperature, heart rate, and respiration rate were normal. Automated blood pressure was difficult to obtain; manual blood pressure was 108/78 mm Hg.
Laboratory evaluation revealed mild hemolytic anemia and thrombocytopenia; the serum albumin level was normal. Serum chemistries showed the following levels: sodium, 130 mEq/L; potassium, 3.0 mEq/L; chloride, 93 mEq/L; carbon dioxide, 28 mEq/L; blood urea nitrogen, 24 mg/dL; and creatinine, 0.4 mg/dL. Urinalysis results showed moderate blood and greater than 300 mg/dL protein; urine protein-to-creatinine ratio was 30.5. Antistreptolysin O titer, antinuclear antibody titer, and serum C3 and C4 complement levels were normal.
The patient was hospitalized and given potassium supplements. He persistently resisted blood pressure measurement during the first day of hospitalization. Results of further laboratory workup, including serological testing for an infectious cause of Bell palsy, were negative.
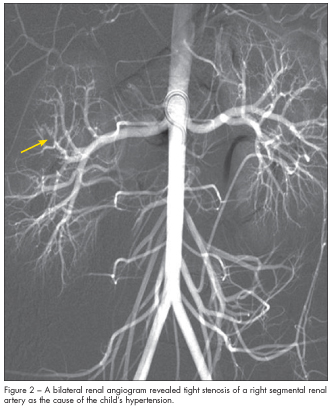 Renal Doppler ultrasonogram was normal. MRI scan of the brain revealed no intracranial pathology. However, while the patient was sedated for the MRI, automated blood pressures were 180/106 mm Hg and 177/110 mm Hg. This prompted an extensive evaluation for secondary hypertension. Results showed a plasma renin level of 4785 ng/dL and a serum aldosterone level of 89 ng/dL. A bilateral renal arteriogram revealed tight stenosis of a right segmental renal artery (Figure 2).
Renal Doppler ultrasonogram was normal. MRI scan of the brain revealed no intracranial pathology. However, while the patient was sedated for the MRI, automated blood pressures were 180/106 mm Hg and 177/110 mm Hg. This prompted an extensive evaluation for secondary hypertension. Results showed a plasma renin level of 4785 ng/dL and a serum aldosterone level of 89 ng/dL. A bilateral renal arteriogram revealed tight stenosis of a right segmental renal artery (Figure 2).
The patient’s hypertension was controlled by gradually increasing the dose of enalapril then adding labetalol. Once his systolic blood pressure had normalized, he underwent alcohol ablation of the right segmental renal artery by interventional radiology. This had no effect on his hypertension, and the child required the same dosages of both enalapril and labetolol for optimal blood pressure control. Two months after the initial procedure, he underwent a second alcohol ablation of the right segmental renal artery. His hypertension is currently controlled with gradually decreasing doses of enalapril only.
RENAL ARTERY STENOSIS
IN CHILDREN
Renal artery stenosis is an important cause of surgically correctable hypertension in children. Renovascular disease accounts for about 5% to 10% of hypertension in children.1 Fibromuscular dysplasia is usually the underlying cause of renal artery stenosis in children and adolescents. Most cases of fibromuscular dysplasia of the renal artery are unilateral, although the disease may be bilateral.2 Renal artery stenosis is associated with several clinical disorders and syndromes in children, including neurofibromatosis type 1, tuberous sclerosis, William syndrome, Marfan syndrome, Takayasu disease, Kawasaki disease, polyarteritis nodosa, moyamoya syndrome, radiation exposure, trauma, umbilical artery catheterization, renal transplant, and congenital rubella syndrome.3-7
Renal artery stenosis should be suspected in children with symptomatic hypertension (irritability,
behavioral changes, headache, lethargy), neurological complications (facial palsy, seizures, intracranial bleeding), or signs of end organ damage (left ventricular hypertrophy, renal insufficiency). The decrease in renal blood flow and intraglomerular pressures from the stenotic renal vessels results in markedly elevated levels of plasma renin and aldosterone. This in turn may cause hypokalemia and persistent hypertension despite treatment with multiple medications. Renal artery stenosis can also present with signs of microangiopathic hemolysis.7
Doppler ultrasonography is a useful screening study for renal artery stenosis. However, it may be insensitive in detecting small branches or accessory renal artery stenosis.8 Intra-arterial digital subtraction angiography is the gold standard—albeit more invasive—test for diagnosing renal artery stenosis.9 Other less invasive diagnostic methods include radionuclide imaging, magnetic resonance angiography, and CT angiography.
BELL PALSY AND HYPERTENSION
The association between facial paralysis and hypertension was first reported in 1869 by Moxon in “Apoplexy into Canal of Fallopius.”10 Moxon described a patient with Bright disease (nephritis) who had a lower motor neuron facial paralysis; dissection of the facial bone revealed a blood clot in the facial canal. Since this description, hypertension has been identified as the cause of facial palsy in many cases.11-14 Renal artery stenosis, like other surgically correctable causes of hypertension, usually presents as moderate to severe hypertension. Patients with renal artery stenosis can be asymptomatic, although some present with Bell palsy, cardiac failure, encephalopathy, or stroke.11 Therefore, clinicians should suspect hypertension in any child who presents with Bell palsy. Identification of hypertension should prompt evaluation for a cause that includes, but is not limited to, renal artery stenosis.
TREATMENT OF RENAL ARTERY
STENOSIS IN CHILDREN
Patients with renovascular hypertension usually have chronic high blood pressure, which must be lowered gradually. Avoid angiotensin-converting enzyme (ACE) inhibitors and angiotensin II receptor blockers (ARBs) until the stenotic vessel is localized. This is because ACE inhibitors and ARBs can reduce an already diminished glomerular filtration pressure and cause severe acute kidney injury in some patients with bilateral severe stenosis, high-grade stenosis in kidney, or chronic kidney disease.15 However, because the renin-angiotensin-aldosterone system is often activated in patients with renal artery stenosis, ACE inhibitors and ARBs may provide better blood pressure control. Moreover, they can minimize proteinuria.16
For patients who cannot tolerate antihypertensive medications or who have hypertension that is refractory to antihypertensive medications, revascularization and restoration of renal blood flow is required.7 Revascularization can be achieved via surgery, segmental transarterial ethanol ablation, or percutaneous angioplasty. Percutaneous angioplasty, with or without stenting, is most commonly used.17 However, in cases of segmental branch stenosis, for which angioplasty is difficult to perform, segmental ethanol ablation may be a reasonable alternative.18 In general, the choice of treatment depends on the age and size of the child, technical feasibility, extent of the disease process, and underlying cause.
1. Wyszynska T, Cichocka E, Wieteska-Klimczak A, et al. A single pediatric center experience with
1025 children with hypertension. Acta Paediatr. 1992;81:244-246.
2. Slovut DP, Olin JW. Fibromuscular dysplasia. N Engl J Med. 2004;350:1862-1871.
3. Hiner LB, Falkner B. Renovascular hypertension in children. Pediatr Clin North Am. 1993;40:
123-140.
4. Choi Y, Kang BC, Kim KJ, et al. Renovascular hypertension in children with moyamoya disease.
J Pediatr. 1997;131:258-263.
5. Fieldston E, Albert D, Finkel T. Hypertension and elevated ESR as diagnostic features of Takayasu arteritis in children. J Clin Rheumatol. 2003;9:156-163.
6. Foster BJ, Bernard C, Drummond KN. Kawasaki disease complicated by renal artery stenosis.
Arch Dis Child. 2000;83:253-255.
7. Tullus K, Brennan E, Hamilton G, et al. Renovascular hypertension in children. Lancet. 2008;371:
1453-1463.
8. Brun P, Kchouk H, Mouchet B, et al. Value of Doppler ultrasound for the diagnosis of renal artery stenosis in children. Pediatr Nephrol. 1997;11:27-30.
9. Dillon MJ. The diagnosis of renovascular disease. Pediatr Nephrol. 1997;11:366-372.
10. Lloyd AV, Jewitt DE, Still JD. Facial paralysis in children with hypertension. Arch Dis Child. 1966;41:292-294.
11. Loggie JM. Evaluation and management of childhood hypertension. Surg Clin North Am. 1985;65:1623-1649.
12. Lorch M, Teach SJ. Facial nerve palsy: etiology and approach to diagnosis and treatment.Pediatr Emerg Care. 2010;26:763-773.
13. Aynaci FM, Sen Y. Peripheral facial paralysis as initial manifestation of hypertension in a child. Turk J Pediatr. 2002;44:73-75.
14. Katusic SK, Beard CM, Wiederholt WC, et al. Incidence, clinical features, and prognosis in
Bell’s palsy, Rochester, Minnesota, 1968-1982. Ann Neurol. 1986;20:622-627.
15. Hricik DE, Browning PJ, Kopelman R, et al. Captopril-induced functional renal insufficiency
in patients with bilateral renal-artery stenoses or renal-artery stenosis in a solitary kidney.
New Engl J Med. 1983;308:373.
16. Kanitkar M. Renovascular hypertension. Indian Pediatr. 2005;42:47-54.
17. König K, Gellermann J, Querfeld U, Schneider MB. Treatment of severe renal artery stenosis by percutaneous transluminal renal angioplasty and stent implantation: review of the pediatric experience: apropos of two cases. Pediatr Nephrol. 2006;21:663-671.
18. Ishijima H, Ishizaka H, Sakurai M, et al. Partial renal embolization for pediatric renovascular
hypertension secondary to fibromuscular dysplasia. Cardiovasc Intervent Radiol. 1997;20:383-386.