
Peer Reviewed
What Is the Cause of This Patient’s Ocular Symptoms?
Authors:
Leonid Skorin Jr, DO, OD, MS, and Emmalee A. Toldo, OD
Citation:
Skorin L Jr, Toldo EA. What is the cause of this patient’s ocular symptoms? Consultant. 2018;58(9):245-248.
An 87-year-old woman presented with a several-month history of persistent swelling and pain of the medial aspect of the right superior eyelid. She reported daily tearing and matter collecting in the corner of her right eye. Her vision was unaffected, and she did not have any photophobia. Artificial tear use did not improve comfort, although she did report mild relief of symptoms with the use of a warm compress over the eyelid. She had been prescribed polymyxin B/trimethoprim ophthalmic medication, 4 times a day in the right eye for 2 weeks, and oral cephalexin, 500 mg 2 times a day for 1 week, with no improvement in symptoms.
She had no history of trauma or surgery to the area, ulceration, or bleeding. She had no recent illness or fever. She had no reported allergies or history of skin cancer. She denied having any new rashes, cold sores, or known exposure to eye infections. She was not a contact lens wearer. She had a history of stage 3 chronic kidney disease, diet-controlled type 2 diabetes, polymyalgia rheumatica, and hypertension, the latter of which was controlled with medication.
Physical examination revealed erythema and edema around the superior punctum of the right superior eyelid (Figure 1). There was expression of mucopurulent matter and multiple small concretions when pressure was applied to the area with a cotton-tip applicator. The surrounding lid tissue and eye showed no injection or sign of allergy. The cornea was clear with no defects. All other ocular and visual findings were normal.

Answer: Canaliculitis
Lacrimal canaliculitis is inflammation of the canalicular tract. It is usually caused by infection of the canaliculus and the proximal lacrimal duct (primary lacrimal canaliculitis) or is secondary to complications of intracanalicular punctal plug or lacrimal stent insertion.1,2
EPIDEMIOLOGY
Lacrimal canaliculitis makes up only 2% to 4% of lacrimal pathologies.1,3,4 It is predominantly unilateral, although bilateral presentation can occur.2,5 The inferior canaliculus is affected in two-thirds of cases, with multiple canalicular involvement in a small percentage of cases either at presentation or in subsequent episodes.2,6 It is more commonly found in women, with a 5:1 female to male predilection reported in several studies.1,7 This is thought to be due to multiple factors, such as changes in hormones during menopause, which can change the quality of tear production and composition.2 Makeup and cosmetics also may contribute to blocked canaliculi and promotion of bacterial growth.2 There is no association with race or ethnicity.1
ETIOLOGY
Primary lacrimal canaliculitis was historically found to be caused by Actinomyces species, a gram-positive rod with fine, branching filaments.1,3,8 Recent studies have reported an increased rate of infection by Staphylococcus and Streptococcus species.1,3 The classic “sulfur granules” or concretions typically associated with Actinomyces israelii infection are not always present in Actinomyces infection and in fact can be formed by other bacteria such as Staphylococcus aureus (Figure 2).1 Other bacterial (eg, Nocardia), fungal (eg, Candida albicans, Fusarium, Aspergillus), or viral (eg, herpes simplex, varicella zoster) entities also can be culprits.1,2,8 Secondary lacrimal canaliculitis, associated with punctal-plug or lacrimal stent use, is commonly caused by Pseudomonas aeruginosa.1,3,8
CLINICAL PRESENTATION
Patients commonly present with pain around the affected area, medial-canthal swelling, persistent unilateral epiphora, recurrent or nonresolving conjunctivitis, and discharge from the punctum.1,2,6,8,9 Classic signs consist of a “pouting” punctum with or without mucopurulent discharge, yellowing of the skin surrounding the canaliculus, and localized hyperemia (Figure 1).1,3 Secondary canaliculitis has also been associated with inflammatory mass projecting from the punctum, and blood-tinged tears or mucopurulent discharge.1,10

NEXT: Diagnosis
DIAGNOSIS
Despite well-described clinical criteria and a prevalence of signs and symptoms, lacrimal canaliculitis is often missed or misdiagnosed, leading to insufficient or ineffective treatment.1,2,9 This commonly causes a prolonged symptomatic period until proper diagnosis is made and definitive treatment is put into effect.2,9 It is important to ask the patient about history of lacrimal stents or previous punctal plug use to determine the possibility of secondary lacrimal canaliculitis.3 Punctal plug placement is a common treatment used for dry eye syndrome.
Although Actinomyces is considered the most common pathogen associated with lacrimal canaliculitis, there is a low success rate in isolating these organisms due to difficulty in culturing and the possibility of polymicrobial infection.1 Microbial culture can consist of conjunctival swabbing, culture of punctal discharge, culture of abscesses, and culture of the concretions (sulfur granules).1 Some physicians will only send for aerobic and anaerobic cultures, while others will culture for bacteria, fungi, and mycobacteria.1 Delayed processing may negatively affect results.1 The number of possible pathogens warrants special instructions to the microbiology laboratory about the need for proper testing.1
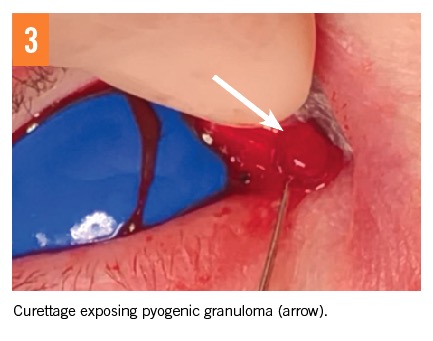
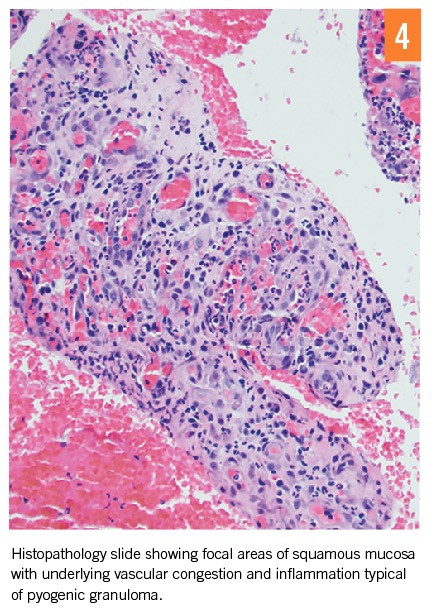
Histopathology of canalicular expression and concretions is the most commonly used diagnostic test.1 Histopathologic findings consistent with pyogenic granuloma have been reported (Figures 3 and 4).1 It is still common for clinicians to diagnose based on histopathology alone.1
Imaging may be helpful for patients who do not present with classical clinical manifestations.4 Use of radiography and radioisotope lacrimal scanning to help confirm diagnosis have been reported.1 Although canalicular imaging by dacryocystography and ultrasound biomicroscopy has been included to help diagnose and document canaliculitis, evidence gathered by clinical examination is sufficient to make a diagnosis in most cases.11,12 In fact, there is a suggestion that not only are these methods unnecessary to make a diagnosis, but also these procedures could cause the canaliculus to form scarring from iatrogenic trauma.7
NEXT: Differential Diagnosis
DIFFERENTIAL DIAGNOSIS
The rate of clinical misdiagnosis ranges from 45% to 100%,3 with multiple misdiagnosis rates of 33% reported in 1 study.7 Watering eyes, intermittent discharge, and pain near the medial canthus are common initial complaints, which can lead to a misdiagnosis of chronic dacryocystitis, chronic conjunctivitis, or rarely a chalazion.2,3 Inflammation noted medially to the lacrimal punctum, and the absence of meibomian glands in this location can help to rule out chalazion.3
Differentiating canaliculitis from dacryocystitis is important. Lacrimal system patency to syringing is typical in canaliculitis, even in the presence of concretions.1 Dacryocystitis will appear in the medial aspect of the inferior eyelid, with more prominent lacrimal sac distention and nasolacrimal duct obstruction.1 Typical treatment for dacryocystitis involves irrigation, which could worsen symptoms of canaliculitis by forcing concretions into more distal portions of the canaliculus.1,7
One must also consider that a neoplasm of the lacrimal system may present with unilateral tearing and masquerade as inflammation.1,13 Carcinoma of the lacrimal canaliculus can include bloody tears, epistaxis, and a mass extending above the medial canthal tendon.13 These characteristics, along with diagnostic histopathologic findings, differentiate it from canaliculitis and emphasize the importance of submitting excised material for histopathologic analysis.13
The aforementioned differential diagnoses emphasize the importance of recognizing the characteristic diagnostic findings of canaliculitis, particularly epiphora, patent lacrimal system, and a swollen, erythematous punctal opening. Presence of mucopurulent discharge or concretions with expression of the punctum, and absence of blood, are also characteristic.
NEXT: Prognosis and Management
PROGNOSIS AND MANAGEMENT
Early recognition and diagnosis of canaliculitis results in better treatment outcomes. Mean duration of symptoms has been reported to be 10 months.1 Medical management has been shown to allow for complete resolution if initiated early in the course of the disease, with best prognosis if symptoms are treated within the first 30 days of symptoms.1,6 For cases of secondary canaliculitis, removal of the lacrimal stent or punctal plug is necessary.1
Medical management includes conservative therapy of oral and topical antibiotics. While antibiotics might improve symptoms temporarily, they do not achieve long-term resolution of symptoms.2 Topical antibiotic therapy alone is associated with a high recurrence rate.2,9 One minimally invasive procedure is intracanalicular irrigation with antibiotic solution.2 Punctal dilation and digital manipulation or expression is another option.2
The prolonged length of time between presentation and accurate diagnosis often results in the formation of concretions deep within the canaliculus.2 The presence of concretions in the canalicular tract is associated with a higher recurrence rate and failure of conservative therapy.4,5 It is postulated that the concretions might obstruct flow of antibiotics and protect bacteria within the granules, allowing the bacteria to survive.1,4,7 The recurrence rate for conservative treatment is 33%.3 When medical management has failed, and for greater long-term success and reduction of recurrences, surgical clearance of the canalicular tracts is recommended.5
Complete removal of the infection and associated concretions requires surgical intervention.1,4,5 Surgical intervention is reported to have a high resolution rate and low recurrence rate.2 In our patient’s case, a canaliculotomy, which is a longitudinal incision along the canaliculus, was performed. Because canaliculotomy allows for greater access to canalicular contents for curettage, it is considered the treatment of choice, with a resolution rate of 80% to 100%, although continued symptoms of epiphora and mattering are common afterwards.1,5,6,7,9,14 The recurrence rate of canaliculitis after surgical management ranges from 0% to 20%.3
Any removed concretions should be collected and sent for microbial culture and histopathologic diagnosis.4,13 Patients should be treated with antibiotic eye drops 4 times daily after surgery. The treatment should be refined after culture results and microbial sensitivity reports return.3,8 If the organism is susceptible to the antibiotic, then the patient should continue using the medication 4 times a day in the affected eye for an additional week.8 If the organism is not susceptible to the initial antibiotic, then a treatment therapy tailored to the results of the microbiology culture and sensitivity should be initiated and continued for 1 to 2 weeks.1,8 Follow-up should continue in 1-week intervals and be guided by clinical findings until complete resolution occurs.2 At 1 week, our patient was asymptomatic, and the incision was healing well (Figure 5).

Leonid Skorin Jr, DO, OD, MS, is an ophthalmologist at the Mayo Clinic Health System in Albert Lea, Minnesota.
Emmalee A. Toldo, OD, is a recent graduate of Pacific University College of Optometry in Forest Grove, Oregon.
REFERENCES:
- Freedman JR, Markert MS, Cohen AJ. Primary and secondary lacrimal canaliculitis: a review of literature. Surv Ophthalmol. 2011;56(4):336-347.
- Kaliki S, Ali MJ, Honavar SG, Chandrasekhar G, Naik MN. Primary canaliculitis: clinical features, microbiological profile, and management outcome. Ophthalmic Plast Reconstr Surg. 2012;28(5):355-360.
- Singh M, Gautam N, Agarwal A, Kaur M. Primary lacrimal canaliculitis—a clinical entity often misdiagnosed. J Curr Ophthalmol. 2018;30:87-90.
- Xiang S, Lin B, Pan Q, et al. Clinical features and surgical outcomes of primary canaliculitis with concretions. Medicine (Baltimore). 2017;96(9):e6188.
- Khu J, Mancini R. Punctum-sparing canaliculotomy for the treatment of canaliculitis. Ophthalmic Plast Reconstr Surg. 2012;28(1):63-65.
- Zaldívar RA, Bradley EA. Primary canaliculitis. Ophthalmic Plast Reconstr Surg. 2009;25(6):481-484.
- Anand S, Hollingworth K, Kumar V, Sandramouli S. Canaliculitis: the incidence of long-term epiphora following canaliculotomy. Orbit. 2004;23(1):19-26.
- Bagheri N, Wajda BN. Canaliculitis. In: Bagheri N, Wajda BN, eds. The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease. 7th ed. Philadelphia, PA: Wolters Kluwer; 2017:138-139.
- Vécsei VP, Huber-Spitzy V, Arocker-Mettinger E, Steinkogler FJ. Canaliculitis: difficulties in diagnosis, differential diagnosis and comparison between conservative and surgical treatment. Ophthalmologica. 1994;208(6):314-317.
- Zaveri J, Cohen AJ. Lacrimal canaliculitis. Saudi J Ophthalmol. 2014;28(1):3-5.
- Hurwitz JJ, Pavlin CJ. Proximal canalicular imaging utilizing ultrasound biomicroscopy B: canaliculitis. Orbit. 1998;17(1):31-36.
- Sathananthan N, Sullivan TJ, Rose GE, Moseley IF. Intubation dacryocystography in patients with a clinical diagnosis of chronic canaliculitis (“streptothrix”). Br J Radiol. 1993;66(785):389-393.
- Charles NC, Lisman RD, Mittal KR. Carcinoma of the lacrimal canaliculus masquerading as canaliculitis. Arch Ophthalmol. 2006;124(3):414-416.
- Kim UR, Wadwekar B, Prajna L. Primary canaliculitis: the incidence, clinical features, outcome and long-term epiphora after snip–punctoplasty and curettage. Saudi J Ophthalmol. 2015;29(4):274-277.