
Peer Reviewed
Nasal Septal Perforation: A Guide for Clinicians
Authors:
Hunter Elms, BS; Minas P. Economides, MD; and Gabriel M. Aisenberg, MD
Department of Internal Medicine, the University of Texas School Health Science Center at Houston McGovern Medical School, Houston, Texas
Citation:
Elms H, Economides MP, Aisenberg GM. Nasal septal perforation: a guide for clinicians. Consultant. 2019;59(8):227-229, 236, 256.
ABSTRACT: Nasal septal perforation, a communication between the nasal passageways, is usually discovered incidentally during clinical or radiological examination. A broad variety of presumed etiologies have been described, making the diagnostic approach heterogeneous. In this review, we present the reported causes and updated diagnostic and therapeutic management recommendations.
KEYWORDS: Nasal septum, perforation, septoplasty, granulomatosis polyangiitis, relapsing polychondritis, cocaine, rhinitis medicamentosa
A nasal septal perforation (NSP) is a communication between nasal passageways via the cartilaginous or bony portions of the nasal septum. The clinical presentation is indolent for the most part, and most patients with NSP are asymptomatic. For this reason, the prevalence has been inferred from reported radiographic incidental findings. For example, a study of a Swedish population demonstrated that 1% of patients screened had radiographic evidence of NSP,1 whereas a US study demonstrated an NSP prevalence of 2% in an urban population undergoing computed tomography scans for other indications.2
Nasal crusting and epistaxis are commonly present in children with NSP, while in adults rhinorrhea and obstruction have also been described.3 The size and location of an NSP influence its presentation: Whistling is a more common sign of a small anterior perforation, whereas a posterior perforation is more likely to form asymptomatic scar tissue.
While most cases of NSP are iatrogenic after a variety of nasal procedures or surgeries, other etiologies are possible, and in some cases NSP is a harbinger of systemic diseases. In this article, we review the reported causes and present diagnostic and therapeutic management recommendations.
ANATOMY
The nasal septum is a trapezoidal plate of bone and cartilage with mucosal overlay that extends posteriorly from the nasal vestibule to the choanae and lies perpendicular to the hard palate in the sagittal plane. An anterior cartilaginous portion abuts the posterior bony portion of the septum; anteriorly, the septal quadrangular cartilage lies superior to the small vomeronasal cartilage, whereas the perpendicular plate of the ethmoid bone sits above the vomer bone posteriorly. Bony crests from the maxilla and palatine bone contribute to the posterior-inferior bony septum (Figure). Histologically, the septum comprises the nasal mucosa overlying the anterior and posterior perichondrium.4
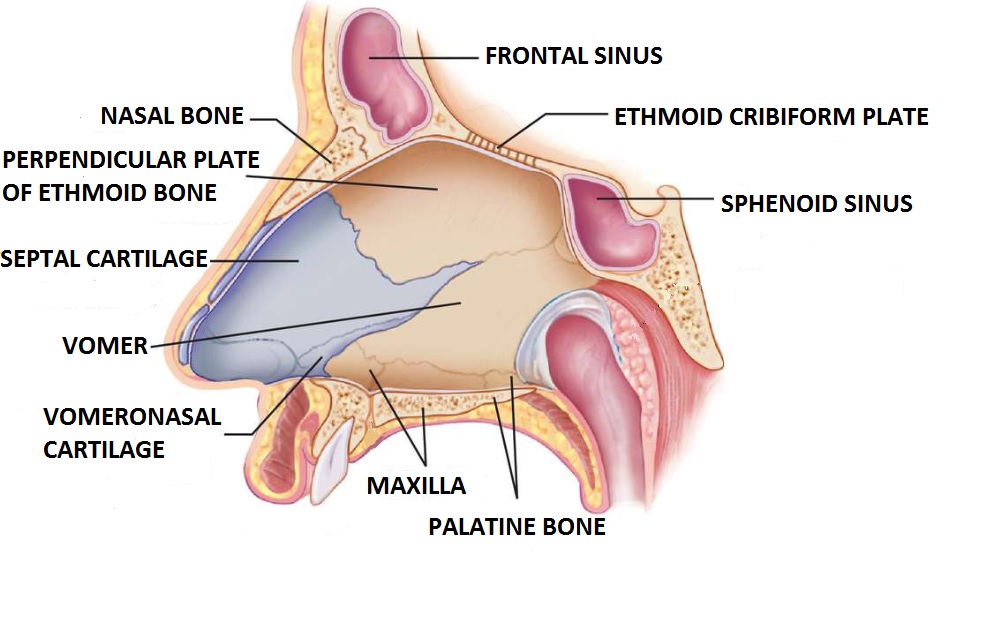
Figure. Anatomy of the nasal septum.
PHYSICAL EXAMINATION
The best way to diagnose an NSP is with direct visualization of the perforation. Caudal nasal perforations can be seen directly with anterior rhinoscopy. Furthermore, illumination of one nostril with a flashlight and observation of the light beam in the other nostril increases the yield of this finding.5
ETIOLOGY
Any insult that separates the mucosa from the perichondrium or interferes with the tenuous blood supply to these structures can lead to degeneration, and eventual perforation of the septum. The Table presents a list of reported causes of NSP.
Table. Reported Causes of Nasal Septal Perforation | |
Trauma | Surgical complications6 |
Nose-picking, rhinotillexomania7-11 | |
Foreign objects, including inhalers12-15 | |
Drugs and Toxins | Cocaine16-19 |
Methamphetamine20 | |
Ketamine21 | |
Vasoconstrictors (rhinitis medicamentosa)22 | |
Intranasal corticosteroids13-15 | |
Industrial irritants (eg, copper, arsenic, chromium, nickel)23-25 | |
Soda ash26 | |
Bevacizumab27 | |
Neoplasms28 | Nasal carcinoma |
Multiple myeloma | |
Non-Hodgkin lymphoma | |
Natural killer cell/nasal cell lymphoma | |
Autoimmune and Inflammatory Causes | Systemic lupus erythematosus28 |
Granulomatosis with polyangiitis28-31 | |
Relapsing polychondritis32,33 | |
Immunoglobulin G4-related disease34,35 | |
Pyoderma gangrenosum36 | |
Takayasu arteritis36 | |
Rheumatoid arthritis36 | |
Mixed connective tissue disorder36 | |
Psoriatic arthritis36 | |
Systemic sclerosis36 | |
Cryoglobulinemia37 | |
Crohn colitis38 | |
Dermatomyositis39 | |
Sarcoidosis40 | |
Infections | Leprosy41,42 |
Tuberculosis43 | |
Nontuberculous mycobacteria44,45 | |
HIV/AIDS46 | |
Histoplasmosis47 | |
Aspergillosis48 | |
Mucor48 | |
Environmental molds48 | |
Mucocutaneous leishmaniasis49 | |
Syphilis50 | |
Congenital Defects of Nasal Bones51 | |
Although the largest group of adult patients with symptomatic perforation have no obvious NSP etiology, iatrogenic causes, especially septoplasty and nasal cautery/packing, account for most cases where a cause is identified.6 Outside of the operating room, nose-picking and its associated compulsive behavior, rhinotillexomania—described in up to 17% of certain adolescent populations—can result in extensive damage not only to the nasal septum, but also to surrounding structures such as the ethmoid sinuses, nasal alae, hard palate, and inferior orbital wall.7-9 Traumatic septal hematomas and posttraumatic abscesses are found predominantly in children.10 This may be due to looser connections between the perichondrium and periosteum and underlying cartilage and bone, allowing for blood pooling between these layers and eventual septal dissolution.11 Foreign bodies, which are common cause of pediatric nasal trauma and obstruction, rarely cause NSP.12
Numerous pharmacological substances are linked with NSP. The mechanisms of septal damage caused by these substances range from vasoconstrictive ischemia to direct cytotoxicity. Overall, cocaine use is the most common etiology of NSP.16 Lateral nasal wall destruction or involvement of the hard palate have been described as a cocaine-induced midline destructive lesion syndrome.17,18
Vasoconstriction is the underlying mechanism that leads to NSP. Over time, chronic ischemia results in tissue necrosis of the perichondrium and periosteum. Chemical irritation by a variety of substances used to cut cocaine (eg, talc, mannitol, lactose, borax) may further contribute to septal damage.19 Other vasoactive drugs of abuse, such as methamphetamine and ketamine, can also lead to NSP.20,21
Nasal decongestants such as phenylephrine and oxymetazoline may also cause local vasoconstriction and septal perforation. Longer than 5 days of use can induce rhinitis medicamentosa, and chronic use can induce nasal polyps and ethmoiditis.22
The use of intranasal corticosteroids is also linked with NSP, notably in female patients within 12 months of initiation of therapy.13 Beclomethasone is the intranasal corticosteroid observed to most commonly cause crusting and/or epistaxis preceding perforation.14 Numerous mechanisms linking local corticosteroids and NSP are postulated but have yet to be confirmed, ranging from local vasoconstriction by inhibition of inflammatory vasodilators to mechanical trauma caused by fluid jets.15
Industrial exposure to irritants such as chromium compounds, copper, arsenic, and nickel has been described as a cause of NSP.23,24 Rhinitis leading to epistaxis is the most common clinical presentation.25 Workers chronically exposed to large quantities of soda ash without protective equipment had rates of perforation reportedly as high as 12%.26
The use of bevacizumab, a monoclonal antibody that inhibits the expression of vascular endothelial growth factor A, approved to treat hereditary hemorrhagic telangiectasia and some advanced solid tumors, is also associated with NSP.27
Non-Hodgkin lymphoma, skin basal and squamous cell carcinoma, and melanoma have been described as causes of NSP. Also, patients with the very rare natural killer/nasal cell lymphoma, prevalent in Asia and Latin America, can present with epistaxis and ulceration mimicking an invasive fungal infection, leading to NSP and death within 5 years in 80% of patients.52 Tissue biopsy is essential for the diagnosis of these diseases.
The nasal mucoperichondrium and periosteum, rich in vascular structures, are subject to vasculitic insults, whereas the cartilaginous structures of the nose itself can be the target of autoimmune diseases. Among the autoimmune etiologies of NSP, granulomatosis with polyangiitis (GPA) is the leading cause of perforations (48% of cases), followed by relapsing polychondritis (26%) and systemic lupus erythematosus (6%). Besides NSP, GPA is associated with destructive lesions of the paranasal sinuses, pharynx, and larynx, and vasculitis affecting the lungs, kidneys, and upper aerodigestive tract.28 Nasal manifestations range from nasal crusting, sinusitis, obstruction, and epistaxis in most patients; epiphora, nasal perforation, and orbital pseudotumor occur in rare cases.29 In extreme cases, saddle-nose deformity, an extreme form of NSP whereby nasal bridge support mechanisms are eroded and external deformity results, can be observed.30 Additionally, sinonasal GPA can present in association with relapsing polychondritis, an autoimmune condition in which auricular, nasal, laryngeal, and joint cartilage becomes periodically and painfully inflamed and destroyed.32 As many as 25% of patients with relapsing polychondritis demonstrate antineutrophil cytoplasmic antibody (ANCA) positivity.33 Tissue pathology, not always used for diagnosis, allows some differentiation of these conditions. Treatment is directed at GPA, as this is generally considered more severe than relapsing polychondritis.31
Immunoglobulin G4-related disease (IgG4-RD) is characterized by infiltrative IgG4-positive plasma cells, obliterative phlebitis, and fibrosis, and it represents a common disease process for a number of conditions previously described as distinct entities.34 Sinonasal compromise in IgG4-RD includes palatal erosion and vomero-ethmoid destruction.35
Mycobacterium leprae is the most common mycobacterium causing NSP, with the nasal mucosa being involved in up to 95% of patients with lepromatous leprosy.41,42 Clinical manifestations can range from epistaxis to NSP to total destruction of the nasal septum. The overall clinical picture of lepromatous leprosy usually supports the diagnosis. Primary nasal tuberculosis has been rarely reported.43 Nasal mucosa biopsy is necessary for diagnosis of this form of disseminated tuberculosis. Radiological evaluation of lung involvement is essential. Other mycobacteria, such as Mycobacterium kansasii and Mycobacterium marinum, are rarely reported causes of NSP.44,45
Although some case reports have described NSP in patients with AIDS and chronic rhinosinusitis, the mechanism of NSP development in these patients is unclear.46 Furthermore, in patients with AIDS, invasive fungal infections including with Histoplasma capsulatum can cause nasal ulcers and perforation.47 Mucocutaneous leishmaniasis, which is most common in South America, can cause tumors and eventually perforation of the septum, months to years after a frequently unapparent fly bite carrying the parasite. Histopathological analysis of the nasal mucosa is essential for diagnosis, and new polymerase chain reaction techniques add some diagnostic help.49 Rarely, tertiary syphilis can destroy the cartilaginous portion of the septum. A combination of serology and histology (endarteritis and plasma cell infiltrates) are diagnostic.50
DIAGNOSIS AND WORKUP
Perhaps because of its infrequent presentation, diagnostic guidelines for NSP are lacking. History and physical examination are the most important tools in a clinician’s arsenal to diagnose its presence. When NSP is suspected, a detailed history should be obtained regarding prior surgeries, trauma to the nose, drug use, and any rheumatologic symptoms. Direct visualization with the help of a flashlight is usually enough to find a caudal NSP. In contrast, when no obvious cause is found, when rapid enlargement of the NSP occurs, and when the condition appears in immunocompromised hosts, an examination by an otolaryngologist with tissue biopsy when indicated is recommended.
Biopsy of the edge of a septal perforation has demonstrated value but can sometimes be nondiagnostic. In two retrospective studies, the correlation between clinical and histological findings in patients with NSP or ulcers was poor.53,54 When the suspicion for malignancy is high, and in cases in which serological evidence supports GPA, tissue analysis had demonstrated a higher diagnostic yield. Although imaging studies can show NSP, they seldom identify the cause. In the right clinical setting, chest radiography (to evaluate for sarcoidosis or tuberculosis), rheumatological or infectious diseases laboratory tests, and serum levels of IgG4 may be valuable to diagnose the etiology of NSP.
TREATMENT
Therapeutic strategies for NSP consist of prevention of further progression of the initial disease process and surgical repair of the septal defect. Asymptomatic NSP with stable size usually requires no intervention.
Treatment with cyclophosphamide and prednisone can frequently cause disease remission in patients with sinonasal and systemic manifestations of GPA.55 Similarly, the use of high-dose induction with prednisolone in combination with oral corticosteroid maintenance has resulted in response in patients with IgG4-RD, although addition of corticosteroid-sparing immunosuppression is often required.56 Whereas medical therapy for systemic causes of NSP cannot reverse the anatomical defect, it can often reduce associated symptoms. For example, antitubercular therapy reduces nasal crusting and airway obstruction in patients with perforations secondary to mycobacterial disease.57
Surgical repair of septal perforation is typically reserved for patients with obstructive symptoms, airflow disturbances, or nasal whistling in the absence of active septal disease or recently treated head and neck carcinoma. Although description of specific surgical techniques is beyond the scope of this review, the spectrum of septal repair ranges from conservative therapy with nasal saline, topical petroleum jelly, saline irrigations, and nasal buttons to aggressive repair with vascularized local flaps, all with the goal of restoring continuity of intranasal contours and reducing turbulent airflow.58,59
CONCLUSIONS
NSP represents a diagnostic dilemma for the clinician due to its broad etiological differential diagnosis. The prognosis is mostly determined by the underlying process. Diagnosis usually requires a thorough investigation and use of multiple tissue specimens, complemented with some laboratory tests. Despite the introduction of novel molecular tests, no cause is found in many cases, which explains the need for further investigation in this field.
- Oberg D, Akerlund A, Johansson L, Bende M. Prevalence of nasal septal perforation: the Skövde population-based study. Rhinology. 2003;41(2):72-75.
- Gold M, Boyack I, Caputo N, Pearlman A. Imaging prevalence of nasal septal perforation in an urban population. Clin Imaging. 2017;43:80-8
- Lanier B, Kai G, Marple B, Wall GM. Pathophysiology and progression of nasal septal perforation. Ann Allergy Asthma Immunol. 2007;99(6):473-479.
- Kim DW, Egan KK, O'Grady K, Toriumi DM. Biomechanical strength of human nasal septal lining: comparison of the constituent layers. Laryngoscope. 2005;115(8):1451-1453.
- Orient JM. The nose. In: Orient JM. Sapira’s Art & Science of Bedside Diagnosis. 3rd ed. Lippincott Williams & Wilkins; 2005:253.
- Hong S-N, Mutsumay S, Jin HR. Long-term results of combined rhinoplasty and septal perforation repair. JAMA Facial Plast Surg. 2016;18(6):475-480.
- Caruso RD, Sherry RG, Rosenbaum AE, Joy SE, Chang JK, Sanford DM. Self-induced ethmoidectomy from rhinotillexomania. AJNR Am J Neuroradiol. 1997;18(10):1949-1950.
- Gigliotti R, Waring HG. Self-inflicted destruction of nose and palate: report of case. J Am Dent Assoc. 1968;76(3):593-596.
- Rathore D, Ahmed SK, Ahluwalia HS, Mehta P. Rhinotillexomania: a rare cause of medial orbital wall erosion. Ophthalmic Plast Reconstr Surg. 2013;29(5):e134-e135.
- Andrade C, Srihari BS. A preliminary survey of rhinotillexomania in an adolescent sample. J Clin Psychiatry. 2001;62(6):426-431.
- Sayin I, Yazici ZM, Bozkurt E, Kayhan FT. Nasal septal hematoma and abscess in children. J Craniofac Surg. 2011;22(6):e17-e19.
- Abou-Elfadl M, Horra A, Abada R-L, Mahtar M, Roubal M, Kadiri F. Nasal foreign bodies: results of a study of 260 cases. Eur Ann Otorhinolaryngol Head Neck Dis. 2015;132(6):343-346.
- Cervin A, Andersson M. Intranasal steroids and septum perforation—an overlooked complication? A description of the course of events and a discussion of the causes. Rhinology. 1998;36(3):128-132.
- Schoelzel EP, Menzel ML. Nasal sprays and perforation of the nasal septum. JAMA. 1985;253(14):2046.
- Benninger MS, Hadley JA, Osguthorpe JD, et al. Techniques of intranasal steroid use. Otolaryngol Head Neck Surg. 2004;130(1):5-24.
- Schwartz RH, Estroff T, Fairbanks DNF, Hoffmann NG. Nasal symptoms associated with cocaine abuse during adolescence. Arch Otolaryngol Head Neck Surg. 1989;115(1):63-64.
- Rubin K. The manifestation of cocaine-induced midline destructive lesion in bone tissue and its identification in human skeletal remains. Forensic Sci Int. 2013;231(1-3):408e1-408e11.
- Kuriloff DB, Kimmelman CP. Osteocartilaginous necrosis of the sinonasal tract following cocaine abuse. Laryngoscope. 1989;99(9):918-924.
- Schweitzer VG. Osteolytic sinusitis and pneumomediastinum: deceptive otolaryngologic complications of cocaine abuse. Laryngoscope. 1986;96(2):206-210.
- Bakhshaee M, Khadivi E, Naseri Sadr M, Esmatinia F. Nasal septum perforation due to methamphetamine abuse. Iran J Otorhinolaryngol. 2013;25(70):53-56.
- Tsai KK, Wang CH. Ketamine-snorting-induced nasal septum perforation. Ear Nose Throat J. 2016;95(7):256.
- Toohill RJ, Lehman RH, Grossman TW, Belson TP. Rhinitis medicamentosa. Laryngoscope. 1981;91(10):1614-1621.
- Krishna G, Mathur JS, Gupta RK. Health hazard amongst chrome industry workers with special reference to nasal septum perforation. Indian J Med Res. 1976;64(6):866-872.
- NIOSH Health Hazard Evaluation Report: HETA #2003-0367-2973. Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health. https://www.cdc.gov/niosh/hhe/reports/pdfs/2003-0367-2973.pdf. Published July 2005. Accessed April 10, 2019.
- Lin SC, Tai CC, Chan CC, Wang JD. Nasal septum lesions caused by chromium exposure among chromium electroplating workers. Am J Ind Med. 1994;26(2):221-228.
- Archibald RM. Perforation of the nasal septum due to soda ash. Br J Ind Med. 1954;11(1):31-37.
- Geltzeiler M, Steele TO. Nasal septal perforation secondary to systemic bevacizumab. Am J Otolaryngol. 2017;38(3):354-355.
- Finkielman JD, Lee AS, Hummel AM, et al; WGET Research Group. ANCA are detectable in nearly all patients with active severe Wegener’s granulomatosis. Am J Med. 2007;120(7):643.e9-643.e14.
- Cannady SB, Batra PS, Koening C, et al. Sinonasal Wegener granulomatosis: a single-institution experience with 120 cases. Laryngoscope. 2009;119(4):757-761.
- Small P, Black M, Davidman M, de Champlain ML, Kapusta MA, Kreisman H. Wegener’s granulomatosis and relapsing polychondritis: a case report. J Rheumatol. 1980;7(6):915-918.
- Guntupalli L, Patel K, Faraji F, Brunworth JD. Autoimmune-related nasal septum perforation: a case report and systematic review. Allergy Rhinol (Providence). 2017;8(1):40-44.
- Papo T, Piette JC, Du LTH, et al. Antineutrophil cytoplasmic antibodies in polychondritis. Ann Rheum Dis. 1993;52(5):384-385.
- File I, Trinn C, Mátyus Z, Ujhelyi L, Balla J, Mátyus J. Relapsing polychondritis with p-ANCA associated vasculitis: which triggers the other? World J Clin Cases. 2014;2(12):912-917.
- Deshpande V, Zen Y, Chan JK, et al. Consensus statement on the pathology of IgG4-related disease. Mod Pathol. 2012;25(9):1181-1192.
- Della-Torre E, Mattoo H, Mahajan VS, et al. IgG4-related midline destructive lesion. Ann Rheum Dis. 2014;73(7):1434-1436.
- Willkens RF, Roth GJ, Novak A, Walike JW. Perforation of nasal septum in rheumatic diseases. Arthritis Rheum. 1976;19(1):119-121.
- Smith I, Smith M, Mathias D, Wallis J. Cryoglobulinaemia and septal perforation: a rare but logical cause. J Laryngol Otol. 1996;110(7):668-669.
- Kriskovich MD, Kelly SM, Jackson WD. Nasal septal perforation: a rare extraintestinal manifestation of Crohn’s disease. Ear Nose Throat J. 2000;79(7):520-523.
- Martinez-Cordero E, Lasky D, Katona G. Nasal septal perforation in dermatomyositis. J Rheumatol. 1986;13(1):231-232.
- Baum ED, Boudousquie AC, Li S, Mirza N. Sarcoidosis with nasal obstruction and septal perforation. Ear Nose Throat J. 1998;77(11):896-898.
- Alobid I, Guilemany JM, Mullol J. Nasal manifestations of systemic illnesses. Curr Allergy Asthma Rep. 2004;4(3):208-216.
- Chaptini C, Marshman G. Leprosy: a review on elimination, reducing the disease burden, and future research. Lepr Rev. 2015;86(4):307-315.
- Khan S, Pujani M, Jetley S. Primary nasal tuberculosis: resurgence or coincidence—a report of four cases with review of literature. J Lab Physicians. 2017;9(1):26-30.
- Bennett AMD, Patel N, Kotecha B, Al-Okati A. Septal perforation secondary to Mycobacterium kansasii infection. J Laryngol Otol. 2003;117(12):992-994.
- Asakura T, Ishii M, Kikuchi T, et al. Disseminated Mycobacterium marinum infection with a destructive nasal lesion mimicking extranodal NK/T cell lymphoma: a case report. Medicine (Baltimore). 2016;95(11):e3131.
- Rejali SD, Simo R, Saeed AM, de Carpentier J. Acquired immune deficiency syndrome (AIDS) presenting as a nasal septal perforation. Rhinology. 1999;37(2):93-95.
- Jaimes A, Muvdi S, Alvarado Z, Rodríguez G. Perforation of the nasal septum as the first sign of histoplasmosis associated with AIDS and review of published literature. Mycopathologia. 2013;176(1-2):145-150.
- Sardana K, Goel K. Nasal septal ulceration. Clin Dermatol. 2014;32(6):817-826.
- Brahn E, Pegues DA, Yao Q, Craft N. Mucocutaneous leishmaniasis masquerading as Wegener granulomatosis. J Clin Rheumatol. 2010;16(3):125-128.
- Prasad BK, Mokamati S. Tertiary nasal syphilis: rare but still a reality. Arch Otolaryngol Rhinol. 2016;2(1):13-15.
- Valencia MP, Castillo M. Congenital and acquired lesions of the nasal septum: a practical guide for differential diagnosis. Radiographics. 2008;38(1):205-224.
- Reategui Schwarz E, Oikonomou KG, Reynolds M, Kim J, Balmiki RL, Sterling SA. Extranodal NK/T-cell lymphoma, nasal type, presenting as refractory Pseudomonas aeruginosa facial cellulitis. J Investig Med High Impact Case Rep. 2017;5(3):2324709617716471.
- Diamantopoulos II, Jones NS. The investigation of nasal septal perforations and ulcers. J Laryngol Otol. 2001;115(7):541-544.
- Murray A, McGarry GW. The clinical value of septal perforation biopsy. Clin Otolaryngol Allied Sci. 2000;25(2):107-109.
- Fauci AS, Haynes BF, Katz P, Wolff SM. Wegener’s granulomatosis: prospective clinical and therapeutic experience with 85 patients for 21 years. Ann Intern Med. 1983;98(1):76-85.
- Ebbo M, Daniel L, Pavic M, et al. IgG4-related systemic disease: features and treatment response in a French cohort: results of a multicenter registry. Medicine (Baltimore). 2012;91(1):49-
- Lai T-Y, Liu P-J, Chan L-P. Primary nasal tuberculosis presenting with septal perforation. J Formos Med Assoc. 2007;106(11):953-955.
- Mullace M, Gorini E, Sbrocca M, Artesi L, Mevio N. Management of nasal septal perforation using silicone nasal septal button. Acta Otorhinolaryngol Ital. 2006;26(4):216-218.
- Re M, Paolucci L, Romeo R, Mallardi V. Surgical treatment of nasal septal perforations. Our experience. Acta Otorhinolaryngol Ital. 2006;26(2):102-109.