
Peer Reviewed
Fibroepithelial Polyp: An Unusual Cause of Acute Urinary Retention in a 5-Year-Old Boy
AUTHORS:
Matthias Manuel, MD, MPH1,2 • Shahid Nadeem, MD1,2 • Elisabeth Moredock, MD1,2 • Dinesh Rakheja, MD1,2 • Susan Scott, MD1,2
AFFILIATIONS:
1University of Texas Southwestern Medical Center, Dallas, Texas
2Children’s Medical Center, Dallas, Texas
CITATION:
Manuel M, Nadeem S, Moredock E, Rakheja D, Scott S. Fibroepithelial polyp: an unusual cause of acute urinary retention in a 5-year-old boy. Consultant. 2021;61(7):e30-e32. doi:10.25270/con.2020.11.00007
Received July 14, 2020. Accepted October 24, 2020. Published online November 5, 2020.
DISCLOSURES:
The authors report no relevant financial relationships.
CORRESPONDENCE:
Matthias Manuel, MD, MPH, Department of Pediatrics, Division of Pediatric Emergency Medicine, Children’s Medical Center, 1935 Medical District Dr, E2.03, Dallas, TX 75235 (matthias.manuel@utsouthwestern.edu)
A 5-year-old previously healthy circumcised boy with no significant history presented to the pediatric emergency department (ED) with a 3-day history of progressively worsening difficulty with urination, poor urinary stream, and urinary retention. Urinalysis (UA) performed at the patient’s primary care provider’s office showed microscopic hematuria with proteinuria, prompting ED referral for further evaluation.
The boy’s mother denied a history of fever, gross hematuria, urethral discharge, constipation, trauma, urinary tract infection (UTI), surgery, spinal cord injuries, nephrolithiasis, urinary retention, or urethral instrumentation or foreign body insertion. There was no significant family history related to his presenting symptoms and no current medication use.
At triage, the patient was quite uncomfortable and had a strong urge to urinate but only made a few drops of urine. His vital signs and physical examination findings were normal, except for suprapubic fullness with some discomfort on palpation. A bedside bladder ultrasonography scan revealed approximately 409 mL of urine, although his expected bladder capacity for age based on the Koff formula ([age in years + 2] × 30) was approximately 210 mL.
The patient was administered acetaminophen for suprapubic discomfort, and transurethral catheterization of his bladder was performed, yielding 300 mL of urine, with a postcatherization bladder scan showing approximately 147 mL of residual urine.
Results of UA done in the ED showed 2+ protein and 37 red blood cells on microscopy. Results of a complete blood cell count; a comprehensive metabolic panel; assessment of serum phosphorus, magnesium, uric acid, and lactate dehydrogenase levels; and a coagulation profile were all normal.
Ultrasonography of the kidneys and bladder revealed a 1.3 × 2.5 × 1.2-cm tubular mass arising from the posterior base of the bladder, adjacent to the prostate, and extending into the bladder lumen (Figures 1 and 2).

Figure 1. Ultrasonogram of the bladder demonstrating a tubular mass at the base of the bladder.

Figure 2. Ultrasonogram of the bladder showing internal color Doppler signal within the mass.
Further imaging studies to better delineate the mass were suggested based on concerns expressed by the radiologist. A follow-up computed tomography (CT) scan (Figure 3) demonstrated an enhancing tubular mass arising from the posterior inferior aspect of the right bladder wall, measuring approximately 2.8 cm. There was minimal diffuse bladder wall thickening without evidence of extravesical extension. Some mildly prominent periaortic and retroperitoneal lymph nodes measuring approximately 7 mm were also noted.
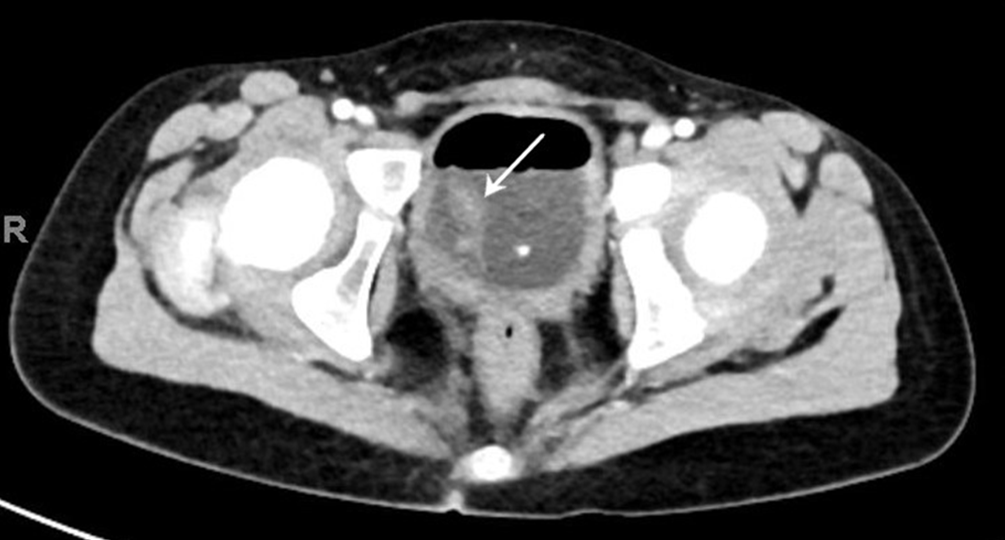
Figure 3. Contrast-enhanced axial CT image of the bladder showing the mass on a thin stalk (arrow).
A urologist was consulted, and given the above findings, a Foley catheter was placed for urinary drainage, and the patient was prepared for cystoscopy with transurethral resection (TUR). During surgical resection, a large, 3- to 4-cm mass, arising just proximal to the prostatic verumontanum on a thin stalk, was noted and excised.
Histopathologic examination of the excised mass showed fibrovascular and muscular tissue with focally preserved urothelial lining and foci of granulation tissue, despite extensive cautery artifact (Figures 4 and 5). No atypical cellular infiltrates were noted.

Figure 4. Photomicrograph showing cauterized fibromuscular tissue lined by focally preserved urothelium (arrow). No atypical cellular infiltrates are noted (hematoxylin-eosin, original magnification ×40).

Figure 5. Photomicrograph showing the focally preserved, benign-appearing urothelial lining with adjacent cautery artifact (hematoxylin-eosin, original magnification ×200).
Discussion. The differential diagnosis of an anatomic mass at the bladder base causing dramatic urinary obstruction and retention in a previously healthy child includes hemangioma, leiomyoma, benign bladder polyp, urethral cyst or polyp, rhabdomyosarcoma, neurofibroma, urinary bladder cystitis cystica, ureterocele, posterior urethral valves, persistent müllerian remnant, transitional cell carcinoma, and adenocarcinoma.1-6
In our patient’s case, in addition to the transurethral cystoscopic surgical findings, the histopathologic report of fibrovascular and muscular tissue with focally preserved urothelial lining and foci of granulation tissue was compatible with a diagnosis of benign fibroepithelial polyp (FEP) of the bladder base.
FEPs are one of the few benign lesions of the genitourinary tract known to be associated with acute urinary tract obstruction, among other symptoms. More than 90% of urothelial tumors are malignant, so concerns about a possible neoplastic etiology is warranted.1
FEP of the genitourinary system is a rare benign tumor of mesodermal origin in infants and children. Although FEPs can occur in any age, they are more common in the third and fourth decades of life with a male preponderance (male to female ratio, 1.5 to 1).4 Most cases (68%-87%) occur as solitary lesions in the proximal ureteropelvic/renal pelvic junction with left-sided predominance. FEPs affecting the bladder and/or urethra are quite rare.2-7
Histologically, FEPs of the genitourinary system are composed of a core of fibrovascular tissue lined by benign urothelium.2,4 They are usually solitary, as seen in this patient’s case, but cases of multiple isolated polyps have been reported.5,8 The cause is unknown; however, etiologic postulates include slow-growing congenital benign lesions or lesions arising from chronic urothelial inflammatory irritants such as infection or obstruction.
The clinical presentation depends on the size and site of the polyp, and symptoms may include urinary retention from obstruction; intermittent suprapubic, pelvic, or flank pain; or hematuria (gross or microscopic). Large polyps close to the bladder outlet or prostatic verumontanum may have a ball-valve effect, resulting in partial obstructive symptoms with urinary intermittency and a sense of incomplete bladder emptying.9 The most common presenting symptom is intermittent hematuria.5-7 However, in a retrospective cohort study of 16 pediatric patients seen over 35 years, Gleason and Cramer reported an equal proportion (50%) of patients with hematuria and obstructive symptoms.10 There also have been reports of hydronephrosis, especially with ureteral polyps.4,11,12 Our patient presented with acute-onset urinary retention and had microscopic hematuria on UA. There was no report of pelvic pain, flank pain, or gross hematuria, nor findings suggestive of hydronephrosis on ultrasonography or CT evaluation of our patient.
No consensus exists on the best imaging modality for FEP of the bladder or urethra. However, in children presenting with obstructive symptoms, the diagnosis of FEP is first suggested by a voiding cystourethrogram or ultrasound scan, followed by CT scanning or magnetic resonance imaging.13 CT scanning is particularly useful in differentiating FEPs arising from the bladder from those of the lower ureter near the ureterovesical junction.12
Cystoscopy with TUR is the diagnostic and therapeutic standard of care, allowing for final histopathologic evaluation and characterization of the resected mass to differentiate FEP from rhabdomyosarcoma and other malignant lesions of urothelium.2,14
Outcome of the case. Our patient has fared well since his surgery, with no report of symptom relapse. He is on close follow-up by a urologist, despite the excellent prognosis of FEP with low risk of recurrence and no report of malignant transformation.
Summary. Health care providers who treat children need to be aware that FEP is a rare but potential cause of acute urinary retention in children, occasionally presenting with dramatic symptoms of hematuria and urinary obstruction in a previously healthy child without known risk factors. Imaging studies can be used as initial evaluation but cannot provide a definitive diagnosis. Endoscopic resection with histopathologic evaluation is the therapeutic and diagnostic gold standard for this pathology. The prognosis is excellent. There is no known history of malignant transformation, and recurrence is rare.
REFERENCES:
- Wong-You-Cheong JJ, Woodward PJ, Manning MA, Sesterhenn IA. From the Archives of the AFIP: neoplasms of the urinary bladder: radiologic-pathologic correlation. Radiographics. 2006;26(2):553-580. doi:10.1148/rg.262055172
- Agarwal S, Sharma D, Pandey S, Sankhwar S. Benign fibroepithelial bladder polyp: a rare cause of childhood haematuria. BMJ Case Rep. 2018;2018:bcr2018226050. doi:10.1136/bcr-2018-226050
- Ballard DH, Rove KO, Coplen DE, Chen TY, Hulett Bowling RL. Fibroepithelial polyp causing urethral obstruction: diagnosis by cystourethrogram. Clin Imaging. 2018;51:164-167. doi:10.1016/j.clinimag.2018.05.009
- Brummeisl W, Fritsche H-M, Huber E, Wieland WF, Ganzer R. A patient with fibroepithelial polyp of the ureter—a rare condition mimicking malignancy: a case report. Case Rep Urol. 2012;2012:901693. doi:10.1155/2012/901693
- Kaba M, Kaba S, Kaya TY, Eren H, Pirinççi N. A giant pedunculated urothelial polyp mimicking bladder mass in a child: a rare case. Case Rep Pediatr. 2014;2014:935850. doi:10.1155/2014/935850
- Abdessater M, Kanbar A, Khoury JE, et al. Endourologic treatment for a fibroepithelial ureteral polyp protruding from the urethra. J Surg Case Rep. 2019;2019(11):rjz320. doi:10.1093/jscr/rjz320
- Keçeli AM, Dönmez Mİ, Kılınç ANU. Fibroepithelial polyp at the bladder neck presenting with gross hematuria in a 5-year-old boy. J Endourol Case Rep. Published online September 17, 2020. doi:10.1089/cren.2019.0125
- Childs MA, Umbreit EC, Krambeck AE, Sebo TJ, Patterson DE, Gettman MT. Fibroepithelial polyps of the ureter: a single-institutional experience. J Endourol. 2009;23(9):1415-1419. doi:10.1089/end.2009.0403
- Daneshmand S. Adenomatous polyp of the verumontanum causing bladder outlet obstruction. ScientificWorldJournal. 2004;4(suppl 1):89-91. doi:10.1100/tsw.2004.51
- Gleason PE, Kramer SA. Genitourinary polyps in children. Urology. 1994;44(1):106-109. doi:10.1016/s0090-4295(94)80018-9
- Chaker K. Benign fibroepithelial polyp of the ureter: a case report. Urol Case Rep. 2018;22:15-16. doi:10.1016/j.eucr.2018.09.021
- Bellin M-F, Springer O, Mourey-Gerosa I, et al. CT diagnosis of ureteral fibroepithelial polyps. Eur Radiol. 2002;12(1):125-128. doi:10.1007/s003300100933
- Isaac J, Snow B, Lowichik A. Fibroepithelial polyp of the prostatic urethra in an adolescent. J Pediatr Surg. 2006;41(12):e29-e31. doi:10.1016/j.jpedsurg.2006.09.066
- Aita GA, Begliomini H, Mattos D Jr. Fibroepithelial polyp of the urethra. Int Braz J Urol. 2005;31(2):155-156. doi:10.1590/s1677-55382005000200012