
Peer Reviewed
COVID-19-Induced Cardiomyopathy
AUTHORS:
Emmanuel S. Santiago, MD1 • Zekarias T. Asnake, MD2 • George H. Cockey, MD, PhD3
AFFILIATIONS:
1University of Central Florida, School of Medicine, Orlando, Florida
2Department of Internal Medicine, University of Central Florida, Orlando, Florida
3Department of Internal Medicine, North Florida Regional Medical Center, Gainesville, Florida
CITATION:
Santiago ES, Asnake ZT, Cockey GH. COVID-19-induced cardiomyopathy. Consultant. 2022;62(3):e28-e30. doi:10.25270/con.2021.06.00013
Received January 24, 2021. Accepted March 5, 2021. Published online June 25, 2021.
DISCLOSURES:
The authors report no relevant financial relationships.
CORRESPONDENCE:
George H. Cockey, MD, PhD, North Florida Regional Medical Center, 6500 West Newberry Road, Gainesville, FL 32605 (GHCGOLFER@MSN.com)
A 58-year-old man presented to the emergency department with a 1-week history of shortness of breath, cough, and wheezing. His medical history was significant for chronic obstructive pulmonary disease (COPD) and confirmed COVID-19 infection 4 weeks prior to presentation, which had self-resolved at home.
A physical examination revealed tachypnea and bilateral lung wheezing without signs of jugular vein distension or lower extremity edema. He was admitted to the hospital with a suspected COPD exacerbation.
Diagnostic testing. Results of a laboratory workup were unremarkable and included a normal troponin level. A COVID-19 polymerase chain reaction (PCR) test returned negative results. Blood test results were negative for viral antibodies (including Coxsackie B, adenovirus, and echovirus) and inflammatory markers.
Results of a chest radiography scan showed no signs of fluid overload, and results of a chest computed tomography scan were negative for pulmonary embolism. An electrocardiogram revealed no significant abnormalities. An echocardiogram demonstrated a reduced ejection fraction of 35% to 40% and diffuse hypokinesis with no evidence of apical ballooning. The echocardiogram was compared with an echocardiogram obtained 2 months earlier, which had demonstrated normal systolic function with an ejection fraction of 55% to 60% and no wall motion abnormality.
A cardiologist was consulted and recommended a left heart catheterization to evaluate this new-onset cardiomyopathy. Results of the catheterization revealed widely patent coronary arteries and confirmed nonischemic cardiomyopathy with an ejection fraction of 35% to 40% (Figures 1 and 2).

Figure 1. Patent left anterior descending artery
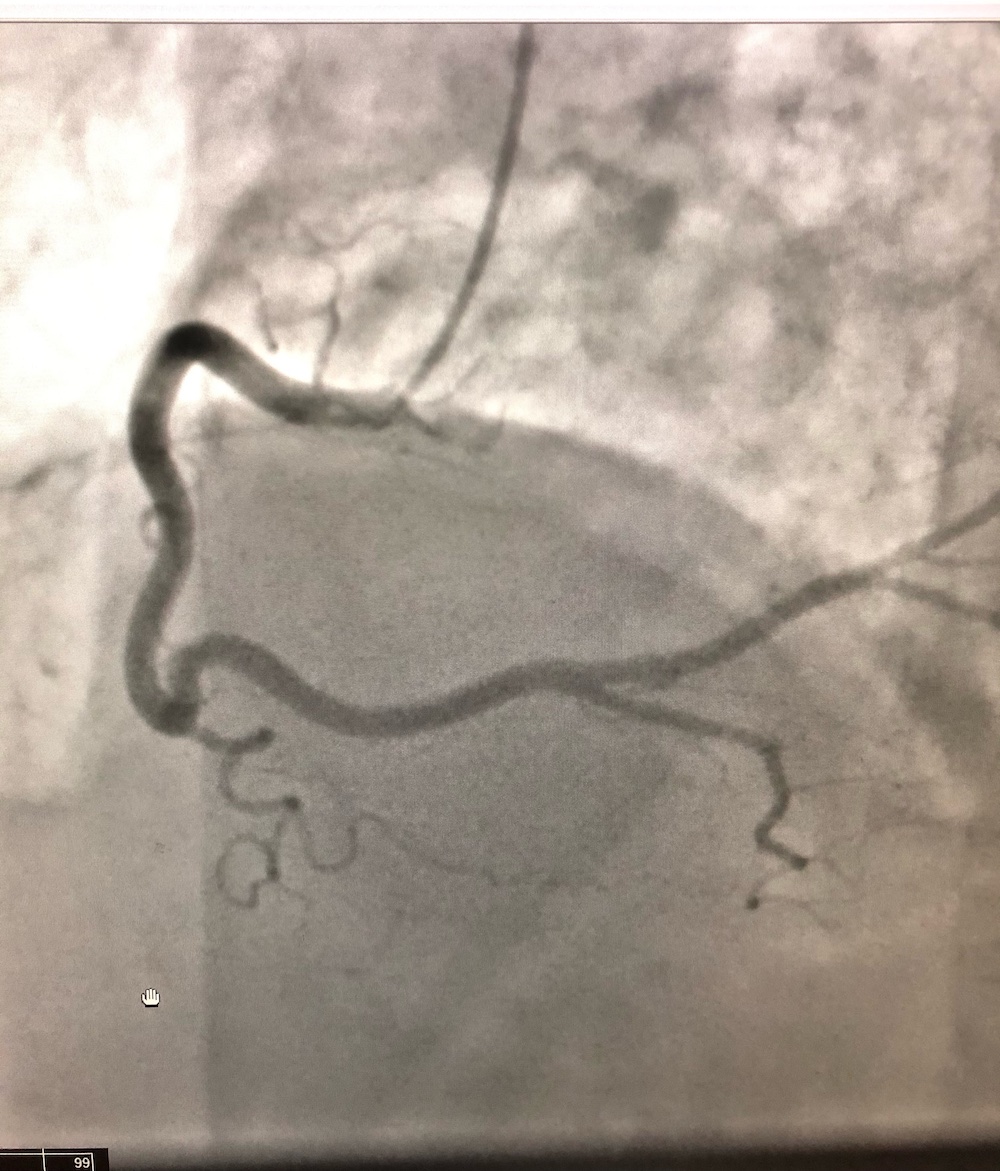
Figure 2. Patent right coronary artery
Discussion. The novel respiratory syndrome COVID-19 has been known to cause significant cardiovascular complications—including arrhythmias, acute coronary syndrome, and myocarditis—during the acute phase of infection in patients with severe illness.1 The exact mechanism in which the SARS-CoV-2 virus causes multiple cardiovascular complications is unknown but may include systemic inflammatory response through cytokine storm, leading to indirect myocardial injury.1
The cardiovascular complications after the recovery phase of infection are not well described. The most reported complication after COVID-19 infection is myocarditis.2 This finding has been reported in patients regardless of preexisting cardiovascular disease status.2 Additionally, it has been reported that the severity of the viral infection, the course of the disease, and presence of cardiac symptoms do not correlate to the signs of myocarditis after recovery from COVID-19 infection.3
Myocarditis can lead to increased incidence of ventricular and atrial arrhythmias and heart failure. Because of the rising reports of cardiovascular complications after COVID-19 infection, it has been suggested to establish post-COVID-19 cardiac follow-up.4 Measuring biomarkers like troponin and brain natriuretic peptide (BNP) has been proposed to identify the population at highest risk of cardiovascular complications after the viral infection.4
Our patient had had COVID-19 infection 1 month prior to presentation and had normal ejection fraction by echocardiogram 2 months prior to presentation. He then was readmitted to the hospital with a COPD exacerbation and found to have markedly reduced ejection fraction by both echocardiogram and cardiac catheterization and widely patent coronary arteries. Results of viral antibody titers were negative. Therefore, we can say with a high degree of confidence that the loss in contractile capacity of the heart is due to delayed complications of COVID-19 infection.
Cardiac inflammation and viability can be assessed by cardiac magnetic resonance imaging (MRI).5,6 Our cardiologist consultant did not recommend an MRI at that time because a left heart catherization was performed, and a cardiac MRI ultimately was not going to change the course of therapy. The gold standard for assessing myocarditis is endomyocardial biopsy; however, this is usually reserved for patients with fulminant myocarditis (ie, those requiring mechanical circulatory support). Fulminant myocarditis has much higher cardiac mortality and transplantation rates.7 Since our patient had no signs of congestive heart failure, there was no indication for this invasive procedure. Additionally, in most cases of myocarditis associated with COVID-19, cardiac MRI and endomyocardial biopsy are avoided because of infection control reasons.1
Conclusion. Based on this case, cardiomyopathy may occur after recovery of COVID-19 infection in asymptomatic patients. This case also demonstrates that biomarkers such as troponin and BNP might not be elevated during the viral infection and that patients can still develop cardiovascular complications during the recovery phase. Hence, cardiovascular follow-up should not be based on these biomarkers alone, and further evaluation with echocardiography scanning would make assessing for cardiovascular complications after COVID-19 infection more comprehensive and complete.
Patient outcome. At discharge, the patient was started on lisinopril, 5 mg, daily for afterload reduction to improve heart function. The cardiologist had initially recommended metoprolol, 25 mg, twice daily and furosemide, 20 mg, daily in addition to lisinopril, but because of the patient’s history of nonadherence to medication, we prescribed only lisinopril. Short-term follow-up with the cardiologist was also recommended.
References
1. Ranard LS, Fried JA, Abdalla M, et al. Approach to acute cardiovascular complications in COVID-19 infection. Circ Heart Fail. 2020;13(7):e007220. https://doi.org/10.1161/circheartfailure.120.007220
2. Rajpal S, Tong MS, Borchers J, et al. Cardiovascular magnetic resonance findings in competitive athletes recovering from COVID-19 infection. JAMA Cardiol. 2021;6(1):116-118. https://doi.org/10.1001/jamacardio.2020.4916
3. Puntmann VO, Carerj ML, Wieters I, et al. Outcomes of cardiovascular magnetic resonance imaging in patients recently recovered from coronavirus disease 2019 (COVID-19). JAMA Cardiol. 2020;5(11):1265-1273. https://doi.org/10.1001/jamacardio.2020.3557
4. Mitrani RD, Dabas N, Goldberger JJ. COVID-19 cardiac injury: Implications for long-term surveillance and outcomes in survivors. Heart Rhythm. 2020;17(11):1984-1990. https://doi.org/10.1016/j.hrthm.2020.06.026
5. Ferreira VM, Schulz-Menger J, Holmvang G, et al. Cardiovascular magnetic resonance in nonischemic myocardial inflammation: expert recommendations. J Am Coll Cardiol. 2018;72(24):3158-3176. https://doi.org/10.1016/j.jacc.2018.09.072
6. Kim RJ, Fieno DS, Parrish TB, et al. Relationship of MRI delayed contrast enhancement to irreversible injury, infarct age, and contractile function. Circulation. 1999;100(19):1992-2002. https://doi.org/10.1161/01.cir.100.19.1992
7. Ammirati E, Veronese G, Brambatti M, et al. Fulminant versus acute nonfulminant myocarditis in patients with left ventricular systolic dysfunction. J Am Coll Cardiol. 2019;74(3):299-311. https://doi.org/10.1016/j.jacc.2019.04.063